Placental biomarker and fetoplacental Doppler abnormalities are strongly associated with placental pathology in pregnancies with small-for-gestational-age fetus: prospective study.
Objective: Placental dysfunction can result in small-for-gestational age (SGA) or fetal growth restriction (FGR). The aim of this prospective cohort study was to assess the association of the cerebroplacental ratio (CPR) and other more conventional fetoplacental Doppler indices, circulating placental growth factor (PlGF) levels and soluble fms-like tyrosine kinase-1 (sFlt-1)/PlGF ratio, with specific placental abnormalities in a large cohort of pregnancies with an SGA/FGR fetus.
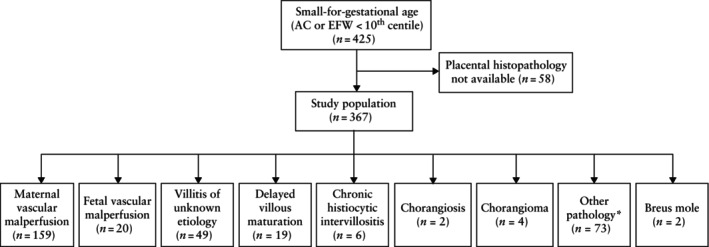
Methods: This was a prospective cohort study of singleton pregnancies with a SGA/FGR fetus conducted at the Centre for Maternal and Fetal Medicine at the Mater Mother's Hospital, Queensland, Australia. Multivariable logistic regression with adjustment for pre-eclampsia was used to evaluate the effect of CPR < 5th centile, umbilical artery Doppler abnormality (defined as umbilical artery (UA) pulsatility index (PI) > 95th centile, or absent or reversed end-diastolic flow), mean uterine artery (UtA) PI > 95th centile and abnormal placental biomarkers (PlGF level < 100 ng/L and sFlt-1/PlGF ratio > 5.78 if gestational age < 28 weeks or > 38 if gestational age ≥ 28 weeks) on the following placental abnormalities, classified based on the Amsterdam Placental Workshop Group Consensus criteria: placental maternal vascular malperfusion (MVM), fetal vascular malperfusion (FVM), villitis of unknown etiology (VUE), chronic histiocytic intervillositis (CHI) and delayed villous maturation (DVM).
Results: Among the 367 women included in this study, MVM was present in 159 (43.3%) placentae, FVM in 20 (5.4%), VUE in 49 (13.4%), DVM in 19 (5.2%) and CHI in six (1.6%). Compared to SGA controls with normal fetoplacental Doppler and placental biomarkers, CPR < 5th centile (adjusted odds ratio (aOR), 3.17 (95% CI, 1.95-5.16); P < 0.001), abnormal UA Doppler (aOR, 2.97 (95% CI, 1.80-4.90); P < 0.001) and mean UtA-PI > 95th centile (aOR, 5.42 (95% CI 2.75-10.70); P < 0.001) were associated with higher odds of placental abnormality. The odds of MVM specifically were significantly higher when CPR < 5th centile (aOR, 2.47 (95% CI, 1.64-4.33); P < 0.001), abnormal UA Doppler (aOR, 3.13 (95% CI, 1.91-5.12); P < 0.001) or mean UtA-PI > 95th centile (aOR, 4.01 (95% CI, 2.25-7.13); P < 0.001) was present. The odds of placental abnormality were also significantly higher if PlGF levels were < 100 ng/L (aOR, 3.66 (95% CI, 2.22-6.06); P < 0.001) or the sFlt-1/PlGF ratio was elevated (aOR, 3.74 (95% CI, 2.17-6.43); P < 0.001). The odds of MVM were also higher in women with PlGF < 100 ng/L (aOR, 2.89 (95% CI, 1.72-4.85); P < 0.001) and elevated sFlt-1/PlGF ratio (aOR, 3.15 (95% CI, 1.83-5.45); P < 0.001).
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


