Gemma Louch, Carl Macrae, Rebecca Talbot, Siobhan McHugh, Jane K O'Hara
{"title":"在实施患者安全事件响应框架之前,英国国家卫生服务系统如何应对、调查和吸取患者安全事件的教训?快速回顾。","authors":"Gemma Louch, Carl Macrae, Rebecca Talbot, Siobhan McHugh, Jane K O'Hara","doi":"10.1097/PTS.0000000000001349","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To understand how National Health Service organizations routinely responded to, investigated, and learned from patient safety incidents in England before the implementation of the Patient Safety Incident Response Framework, and to identify associated success criteria and barriers.</p><p><strong>Methods: </strong>We followed rapid review methodology and searched 2 electronic databases. We aimed to identify and synthesize literature regarding patient safety incident response, investigation, and learning within the English National Health Service, before the implementation of the Patient Safety Incident Response Framework.</p><p><strong>Results: </strong>Nineteen articles were included. A narrative synthesis generated 4 concepts: (1) a multifaceted reporting culture, (2) investigation processes, (3) the landscape of support and involvement, and (4) opportunities to learn. Barriers to incident reporting included time, task characteristics, a culture of blame, and lack of feedback. Root cause analysis was cited as the most common investigation method. Studies outlined points of support and involvement for patients and families, the importance of supporting and involving patients and families, and acknowledged contributions from patients and families may be overlooked currently. For health care staff, the need for timely and personalized support soon after an incident was emphasized. Studies underlined the limitations of current approaches to learning and improvement.</p><p><strong>Conclusions: </strong>These findings lend support to the challenges associated with health care systems' infrastructures and strategies for responding to and learning from patient safety incidents. These challenges centre on 2 interrelated issues: the investigative challenges of rigorously conducting systems analysis and learning-oriented improvement; and the relational challenges of supporting genuine relationships of care, open and honest communication, and supportive engagement after patient safety incidents.</p>","PeriodicalId":48901,"journal":{"name":"Journal of Patient Safety","volume":" ","pages":"e42-e55"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12266792/pdf/","citationCount":"0","resultStr":"{\"title\":\"How Were Patient Safety Incidents Responded to, Investigated, and Learned From Within the English National Health Service Before the Implementation of the Patient Safety Incident Response Framework? A Rapid Review.\",\"authors\":\"Gemma Louch, Carl Macrae, Rebecca Talbot, Siobhan McHugh, Jane K O'Hara\",\"doi\":\"10.1097/PTS.0000000000001349\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To understand how National Health Service organizations routinely responded to, investigated, and learned from patient safety incidents in England before the implementation of the Patient Safety Incident Response Framework, and to identify associated success criteria and barriers.</p><p><strong>Methods: </strong>We followed rapid review methodology and searched 2 electronic databases. We aimed to identify and synthesize literature regarding patient safety incident response, investigation, and learning within the English National Health Service, before the implementation of the Patient Safety Incident Response Framework.</p><p><strong>Results: </strong>Nineteen articles were included. A narrative synthesis generated 4 concepts: (1) a multifaceted reporting culture, (2) investigation processes, (3) the landscape of support and involvement, and (4) opportunities to learn. Barriers to incident reporting included time, task characteristics, a culture of blame, and lack of feedback. Root cause analysis was cited as the most common investigation method. Studies outlined points of support and involvement for patients and families, the importance of supporting and involving patients and families, and acknowledged contributions from patients and families may be overlooked currently. For health care staff, the need for timely and personalized support soon after an incident was emphasized. Studies underlined the limitations of current approaches to learning and improvement.</p><p><strong>Conclusions: </strong>These findings lend support to the challenges associated with health care systems' infrastructures and strategies for responding to and learning from patient safety incidents. These challenges centre on 2 interrelated issues: the investigative challenges of rigorously conducting systems analysis and learning-oriented improvement; and the relational challenges of supporting genuine relationships of care, open and honest communication, and supportive engagement after patient safety incidents.</p>\",\"PeriodicalId\":48901,\"journal\":{\"name\":\"Journal of Patient Safety\",\"volume\":\" \",\"pages\":\"e42-e55\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12266792/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Patient Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/PTS.0000000000001349\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Patient Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/PTS.0000000000001349","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/9 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
How Were Patient Safety Incidents Responded to, Investigated, and Learned From Within the English National Health Service Before the Implementation of the Patient Safety Incident Response Framework? A Rapid Review.
Objective: To understand how National Health Service organizations routinely responded to, investigated, and learned from patient safety incidents in England before the implementation of the Patient Safety Incident Response Framework, and to identify associated success criteria and barriers.
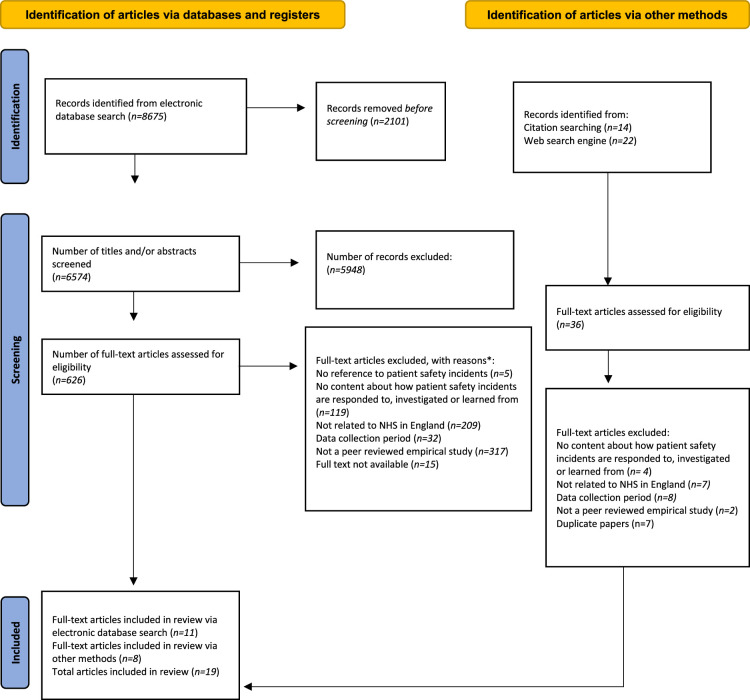
Methods: We followed rapid review methodology and searched 2 electronic databases. We aimed to identify and synthesize literature regarding patient safety incident response, investigation, and learning within the English National Health Service, before the implementation of the Patient Safety Incident Response Framework.
Results: Nineteen articles were included. A narrative synthesis generated 4 concepts: (1) a multifaceted reporting culture, (2) investigation processes, (3) the landscape of support and involvement, and (4) opportunities to learn. Barriers to incident reporting included time, task characteristics, a culture of blame, and lack of feedback. Root cause analysis was cited as the most common investigation method. Studies outlined points of support and involvement for patients and families, the importance of supporting and involving patients and families, and acknowledged contributions from patients and families may be overlooked currently. For health care staff, the need for timely and personalized support soon after an incident was emphasized. Studies underlined the limitations of current approaches to learning and improvement.
Conclusions: These findings lend support to the challenges associated with health care systems' infrastructures and strategies for responding to and learning from patient safety incidents. These challenges centre on 2 interrelated issues: the investigative challenges of rigorously conducting systems analysis and learning-oriented improvement; and the relational challenges of supporting genuine relationships of care, open and honest communication, and supportive engagement after patient safety incidents.
期刊介绍:
Journal of Patient Safety (ISSN 1549-8417; online ISSN 1549-8425) is dedicated to presenting research advances and field applications in every area of patient safety. While Journal of Patient Safety has a research emphasis, it also publishes articles describing near-miss opportunities, system modifications that are barriers to error, and the impact of regulatory changes on healthcare delivery. This mix of research and real-world findings makes Journal of Patient Safety a valuable resource across the breadth of health professions and from bench to bedside.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


