{"title":"银屑病管理中的感染风险和疫苗接种:生物治疗的考虑。","authors":"Laura Mateu-Arrom, Lluis Puig","doi":"10.2147/PTT.S510141","DOIUrl":null,"url":null,"abstract":"<p><p>This narrative review examines critical considerations for biologic treatment in psoriasis patients, with a focus on infection risks, providing current recommendations and practical considerations for prevention, including vaccination, screening, and management strategies. Since type I (Th1) inflammation and type III (Th17) inflammation protect against intracellular and extracellular infections, respectively, it is logical that biologic treatments blocking these pathways may be associated with an increased risk of infection. It has been proven that TNF inhibitors are associated with an increased risk of latent tuberculosis (LTBI) and hepatitis B virus reactivation. However, not all biologics exert the same immunosuppressive effect, as IL-17 and IL-23 inhibitors may be associated with a lower risk of infection. In general, pre-treatment screening for reactivable infectious diseases is advised for all patients initiating biologic therapy. Vaccination schedules for patients with psoriasis under biologic treatment should mirror those of the general population, including annual influenza and COVID-19 vaccines. Live-attenuated vaccines are generally advised against in patients undergoing biologic treatment. However, some live-attenuated vaccines may be safely administered under specific circumstances with IL-17 or IL-23 inhibitors. Current guidelines and recommendations on this topic were initially designed for TNF inhibitors and later extrapolated to other classes of biologic agents. Thus, they should be revised to better align with the specific pathogenic mechanisms of drugs and clinical evidence, emphasizing individualized treatment approaches.</p>","PeriodicalId":74589,"journal":{"name":"Psoriasis (Auckland, N.Z.)","volume":"15 ","pages":"127-144"},"PeriodicalIF":5.2000,"publicationDate":"2025-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998957/pdf/","citationCount":"0","resultStr":"{\"title\":\"Infection Risk and Vaccination in the Management of Psoriasis: Considerations for Biologic Therapy.\",\"authors\":\"Laura Mateu-Arrom, Lluis Puig\",\"doi\":\"10.2147/PTT.S510141\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>This narrative review examines critical considerations for biologic treatment in psoriasis patients, with a focus on infection risks, providing current recommendations and practical considerations for prevention, including vaccination, screening, and management strategies. Since type I (Th1) inflammation and type III (Th17) inflammation protect against intracellular and extracellular infections, respectively, it is logical that biologic treatments blocking these pathways may be associated with an increased risk of infection. It has been proven that TNF inhibitors are associated with an increased risk of latent tuberculosis (LTBI) and hepatitis B virus reactivation. However, not all biologics exert the same immunosuppressive effect, as IL-17 and IL-23 inhibitors may be associated with a lower risk of infection. In general, pre-treatment screening for reactivable infectious diseases is advised for all patients initiating biologic therapy. Vaccination schedules for patients with psoriasis under biologic treatment should mirror those of the general population, including annual influenza and COVID-19 vaccines. Live-attenuated vaccines are generally advised against in patients undergoing biologic treatment. However, some live-attenuated vaccines may be safely administered under specific circumstances with IL-17 or IL-23 inhibitors. Current guidelines and recommendations on this topic were initially designed for TNF inhibitors and later extrapolated to other classes of biologic agents. Thus, they should be revised to better align with the specific pathogenic mechanisms of drugs and clinical evidence, emphasizing individualized treatment approaches.</p>\",\"PeriodicalId\":74589,\"journal\":{\"name\":\"Psoriasis (Auckland, N.Z.)\",\"volume\":\"15 \",\"pages\":\"127-144\"},\"PeriodicalIF\":5.2000,\"publicationDate\":\"2025-04-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998957/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Psoriasis (Auckland, N.Z.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/PTT.S510141\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Psoriasis (Auckland, N.Z.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PTT.S510141","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
Infection Risk and Vaccination in the Management of Psoriasis: Considerations for Biologic Therapy.
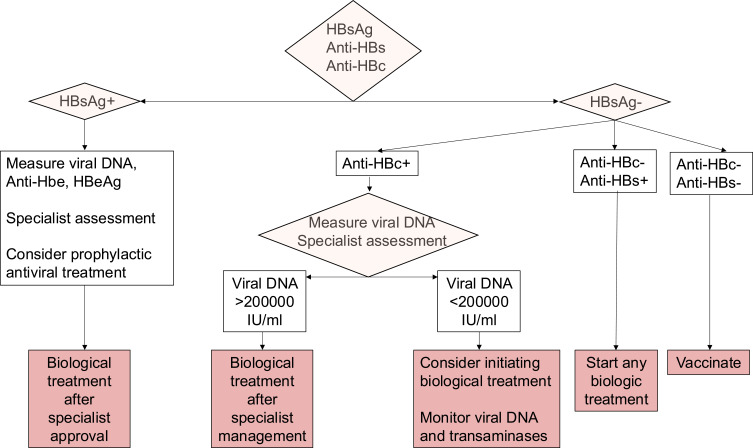
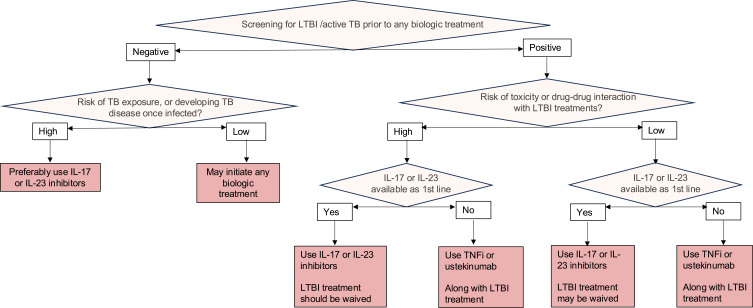
This narrative review examines critical considerations for biologic treatment in psoriasis patients, with a focus on infection risks, providing current recommendations and practical considerations for prevention, including vaccination, screening, and management strategies. Since type I (Th1) inflammation and type III (Th17) inflammation protect against intracellular and extracellular infections, respectively, it is logical that biologic treatments blocking these pathways may be associated with an increased risk of infection. It has been proven that TNF inhibitors are associated with an increased risk of latent tuberculosis (LTBI) and hepatitis B virus reactivation. However, not all biologics exert the same immunosuppressive effect, as IL-17 and IL-23 inhibitors may be associated with a lower risk of infection. In general, pre-treatment screening for reactivable infectious diseases is advised for all patients initiating biologic therapy. Vaccination schedules for patients with psoriasis under biologic treatment should mirror those of the general population, including annual influenza and COVID-19 vaccines. Live-attenuated vaccines are generally advised against in patients undergoing biologic treatment. However, some live-attenuated vaccines may be safely administered under specific circumstances with IL-17 or IL-23 inhibitors. Current guidelines and recommendations on this topic were initially designed for TNF inhibitors and later extrapolated to other classes of biologic agents. Thus, they should be revised to better align with the specific pathogenic mechanisms of drugs and clinical evidence, emphasizing individualized treatment approaches.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


