Ali Rıza Güvercin, Mehmet Orbay Bıyık, Mehmet Aktoklu, Uğur Yazar, Ertuğrul Çakır
{"title":"利用计算机断层扫描引导椎弓根置针定位胸椎病变的新方法的单中心经验。","authors":"Ali Rıza Güvercin, Mehmet Orbay Bıyık, Mehmet Aktoklu, Uğur Yazar, Ertuğrul Çakır","doi":"10.14744/tjtes.2025.82844","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Thoracic level localization in the treatment of thoracic spine problems is more challenging than other spinal regions. The purpose of this study was to prove the reliability of pedicular spinal needle placement under computed tomography guidance before thoracic spine surgery and to reduce the margin of error, surgery time and operating room radiation exposure during thoracic spine and spinal cord surgery.</p><p><strong>Methods: </strong>Fourteen patients undergoing posterior aproach to the thoracic spine and/or spinal cord related lesions were investigated. Spinocaths were placed under CT guidance, into the pedicle of the relevant vertebra, at the same day or the night before surgery. The surgical field is prepared as usual, and a spinocath is placed to the relevant thoracic pedicle under CT guidance.</p><p><strong>Results: </strong>Intraoperative level localization was more reliable and easier in patients undergoing preoperative CT-guided marking in surgeries on the thoracic region performed for various reasons. Shorter preoperative preparation and intraoperative anesthesia times, a decrease in number of fluoroscopic images taken intraoperatively, and no spinal mislocalizations were observed.</p><p><strong>Conclusion: </strong>The results obtained suggest that localising the level with preoperative CT before all types of thoracic surgery is a safe, reliable, and useful method for thoracic spine surgery.</p>","PeriodicalId":94263,"journal":{"name":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","volume":"31 4","pages":"371-374"},"PeriodicalIF":1.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12000984/pdf/","citationCount":"0","resultStr":"{\"title\":\"Single-center experiences with a novel method for preoperative localization of thoracic spine lesions using computed tomography-guided pedicular spinal needle placement.\",\"authors\":\"Ali Rıza Güvercin, Mehmet Orbay Bıyık, Mehmet Aktoklu, Uğur Yazar, Ertuğrul Çakır\",\"doi\":\"10.14744/tjtes.2025.82844\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Thoracic level localization in the treatment of thoracic spine problems is more challenging than other spinal regions. The purpose of this study was to prove the reliability of pedicular spinal needle placement under computed tomography guidance before thoracic spine surgery and to reduce the margin of error, surgery time and operating room radiation exposure during thoracic spine and spinal cord surgery.</p><p><strong>Methods: </strong>Fourteen patients undergoing posterior aproach to the thoracic spine and/or spinal cord related lesions were investigated. Spinocaths were placed under CT guidance, into the pedicle of the relevant vertebra, at the same day or the night before surgery. The surgical field is prepared as usual, and a spinocath is placed to the relevant thoracic pedicle under CT guidance.</p><p><strong>Results: </strong>Intraoperative level localization was more reliable and easier in patients undergoing preoperative CT-guided marking in surgeries on the thoracic region performed for various reasons. Shorter preoperative preparation and intraoperative anesthesia times, a decrease in number of fluoroscopic images taken intraoperatively, and no spinal mislocalizations were observed.</p><p><strong>Conclusion: </strong>The results obtained suggest that localising the level with preoperative CT before all types of thoracic surgery is a safe, reliable, and useful method for thoracic spine surgery.</p>\",\"PeriodicalId\":94263,\"journal\":{\"name\":\"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES\",\"volume\":\"31 4\",\"pages\":\"371-374\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12000984/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14744/tjtes.2025.82844\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/tjtes.2025.82844","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Single-center experiences with a novel method for preoperative localization of thoracic spine lesions using computed tomography-guided pedicular spinal needle placement.
Objective: Thoracic level localization in the treatment of thoracic spine problems is more challenging than other spinal regions. The purpose of this study was to prove the reliability of pedicular spinal needle placement under computed tomography guidance before thoracic spine surgery and to reduce the margin of error, surgery time and operating room radiation exposure during thoracic spine and spinal cord surgery.
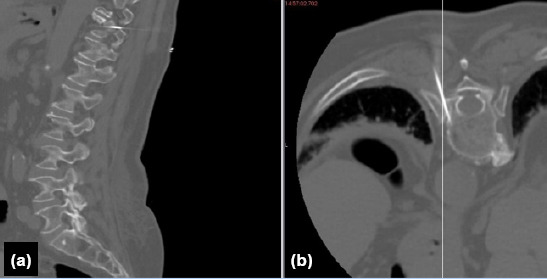
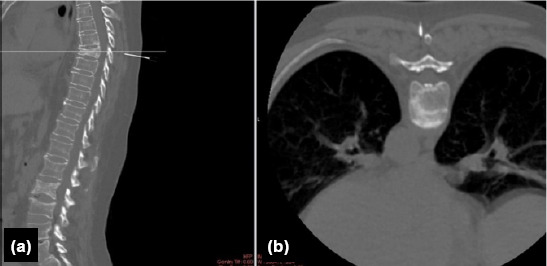
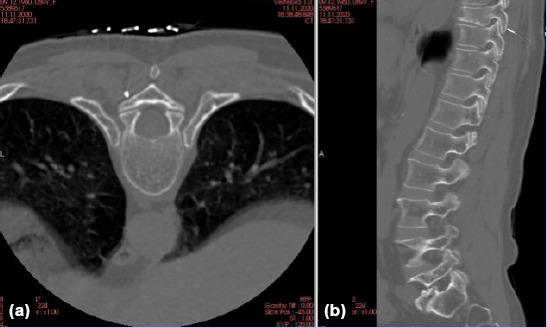
Methods: Fourteen patients undergoing posterior aproach to the thoracic spine and/or spinal cord related lesions were investigated. Spinocaths were placed under CT guidance, into the pedicle of the relevant vertebra, at the same day or the night before surgery. The surgical field is prepared as usual, and a spinocath is placed to the relevant thoracic pedicle under CT guidance.
Results: Intraoperative level localization was more reliable and easier in patients undergoing preoperative CT-guided marking in surgeries on the thoracic region performed for various reasons. Shorter preoperative preparation and intraoperative anesthesia times, a decrease in number of fluoroscopic images taken intraoperatively, and no spinal mislocalizations were observed.
Conclusion: The results obtained suggest that localising the level with preoperative CT before all types of thoracic surgery is a safe, reliable, and useful method for thoracic spine surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


