Revathy Sampath-Kumar, Moman Mohammad, Sacharias von Koch, Ryan Reeves, Belal Al Khiami, Lawrence Ang, Anna Melendez, Ehtisham Mahmud, Ori Ben-Yehuda, David Erlinge
{"title":"实践模式和经皮冠状动脉介入治疗的结果:瑞典和美国的比较。","authors":"Revathy Sampath-Kumar, Moman Mohammad, Sacharias von Koch, Ryan Reeves, Belal Al Khiami, Lawrence Ang, Anna Melendez, Ehtisham Mahmud, Ori Ben-Yehuda, David Erlinge","doi":"10.1093/ehjopen/oeaf045","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Comparisons of international practice patterns and their impact on percutaneous coronary intervention (PCI) outcomes are lacking. We compared temporal PCI trends between Sweden and a large university hospital system in the US.</p><p><strong>Methods and results: </strong>Data within the Swedish Coronary Angiography and Angioplasty Registry (SCAAR) and the University of California San Diego Health internal National Cardiovascular Data Registry (NCDR) CathPCI Registry were used to identify patients who underwent PCI from 2007 to 2021. Baseline characteristics and practice patterns were assessed using all patients (275 021 Swedish cohort, 9883 US cohort). Mortality was analysed using a random-effects Cox model, restricted to patients treated at university hospitals and excluding those with cardiac arrest or cardiogenic shock (108 136 Swedish cohort, 9592 US cohort). The Swedish cohort was older, had a greater proportion of men, and was more likely to smoke (all <i>P</i> < 0.001). The US cohort had a higher body mass index and was more likely to have diabetes, hyperlipidaemia, prior PCI, congestive heart failure, and peripheral arterial disease (all <i>P</i> < 0.001). Sweden had lower rates of PCI for stable angina and lower use of mechanical circulatory support (all <i>P</i> < 0.001). More STEMI patients were treated with only heparin as anticoagulation in Sweden, even in the contemporary era. There was earlier adoption and increased utilization of ticagrelor and radial access in Sweden, while there was earlier use of drug-eluting stents in the US. Fractional flow reserve was used more frequently in Sweden. There was no difference in adjusted all-cause mortality 1 year post-PCI for any indication between university hospitals in Sweden and the US (hazard ratio [HR] 1.09; 95% CI 0.86-1.37; <i>P</i> = 0.48), and this finding was consistent across subgroups.</p><p><strong>Conclusion: </strong>Despite significant differences in patient populations and practice variations, we found no difference in post-PCI mortality between university hospitals in Sweden and the US.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf045"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12053007/pdf/","citationCount":"0","resultStr":"{\"title\":\"Practice patterns and percutaneous coronary intervention outcomes: a comparison between Sweden and the US.\",\"authors\":\"Revathy Sampath-Kumar, Moman Mohammad, Sacharias von Koch, Ryan Reeves, Belal Al Khiami, Lawrence Ang, Anna Melendez, Ehtisham Mahmud, Ori Ben-Yehuda, David Erlinge\",\"doi\":\"10.1093/ehjopen/oeaf045\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Comparisons of international practice patterns and their impact on percutaneous coronary intervention (PCI) outcomes are lacking. We compared temporal PCI trends between Sweden and a large university hospital system in the US.</p><p><strong>Methods and results: </strong>Data within the Swedish Coronary Angiography and Angioplasty Registry (SCAAR) and the University of California San Diego Health internal National Cardiovascular Data Registry (NCDR) CathPCI Registry were used to identify patients who underwent PCI from 2007 to 2021. Baseline characteristics and practice patterns were assessed using all patients (275 021 Swedish cohort, 9883 US cohort). Mortality was analysed using a random-effects Cox model, restricted to patients treated at university hospitals and excluding those with cardiac arrest or cardiogenic shock (108 136 Swedish cohort, 9592 US cohort). The Swedish cohort was older, had a greater proportion of men, and was more likely to smoke (all <i>P</i> < 0.001). The US cohort had a higher body mass index and was more likely to have diabetes, hyperlipidaemia, prior PCI, congestive heart failure, and peripheral arterial disease (all <i>P</i> < 0.001). Sweden had lower rates of PCI for stable angina and lower use of mechanical circulatory support (all <i>P</i> < 0.001). More STEMI patients were treated with only heparin as anticoagulation in Sweden, even in the contemporary era. There was earlier adoption and increased utilization of ticagrelor and radial access in Sweden, while there was earlier use of drug-eluting stents in the US. Fractional flow reserve was used more frequently in Sweden. There was no difference in adjusted all-cause mortality 1 year post-PCI for any indication between university hospitals in Sweden and the US (hazard ratio [HR] 1.09; 95% CI 0.86-1.37; <i>P</i> = 0.48), and this finding was consistent across subgroups.</p><p><strong>Conclusion: </strong>Despite significant differences in patient populations and practice variations, we found no difference in post-PCI mortality between university hospitals in Sweden and the US.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 3\",\"pages\":\"oeaf045\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-04-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12053007/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf045\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf045","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Practice patterns and percutaneous coronary intervention outcomes: a comparison between Sweden and the US.
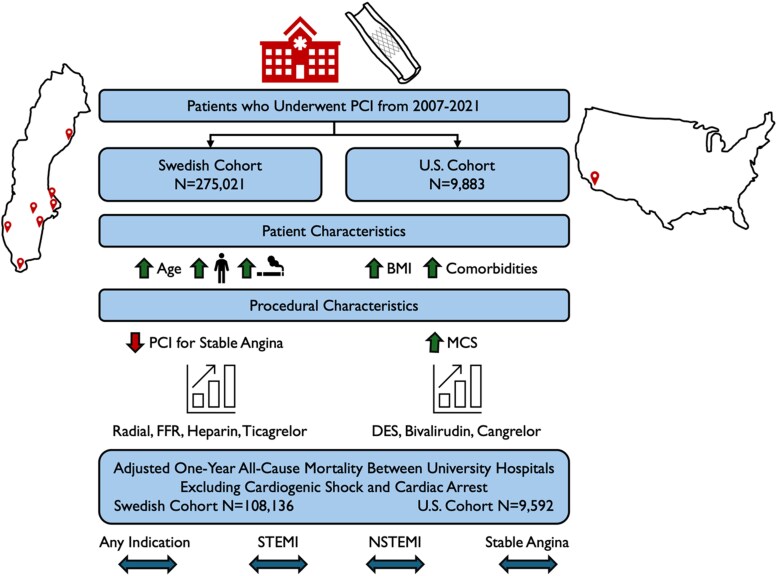
Aims: Comparisons of international practice patterns and their impact on percutaneous coronary intervention (PCI) outcomes are lacking. We compared temporal PCI trends between Sweden and a large university hospital system in the US.
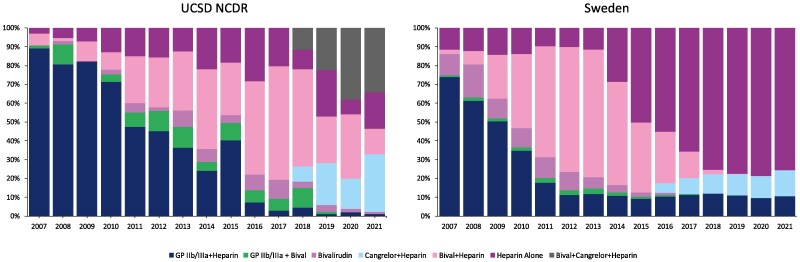
Methods and results: Data within the Swedish Coronary Angiography and Angioplasty Registry (SCAAR) and the University of California San Diego Health internal National Cardiovascular Data Registry (NCDR) CathPCI Registry were used to identify patients who underwent PCI from 2007 to 2021. Baseline characteristics and practice patterns were assessed using all patients (275 021 Swedish cohort, 9883 US cohort). Mortality was analysed using a random-effects Cox model, restricted to patients treated at university hospitals and excluding those with cardiac arrest or cardiogenic shock (108 136 Swedish cohort, 9592 US cohort). The Swedish cohort was older, had a greater proportion of men, and was more likely to smoke (all P < 0.001). The US cohort had a higher body mass index and was more likely to have diabetes, hyperlipidaemia, prior PCI, congestive heart failure, and peripheral arterial disease (all P < 0.001). Sweden had lower rates of PCI for stable angina and lower use of mechanical circulatory support (all P < 0.001). More STEMI patients were treated with only heparin as anticoagulation in Sweden, even in the contemporary era. There was earlier adoption and increased utilization of ticagrelor and radial access in Sweden, while there was earlier use of drug-eluting stents in the US. Fractional flow reserve was used more frequently in Sweden. There was no difference in adjusted all-cause mortality 1 year post-PCI for any indication between university hospitals in Sweden and the US (hazard ratio [HR] 1.09; 95% CI 0.86-1.37; P = 0.48), and this finding was consistent across subgroups.
Conclusion: Despite significant differences in patient populations and practice variations, we found no difference in post-PCI mortality between university hospitals in Sweden and the US.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


