Assessment of risk for pre-eclampsia at mid-gestation to define subsequent care.
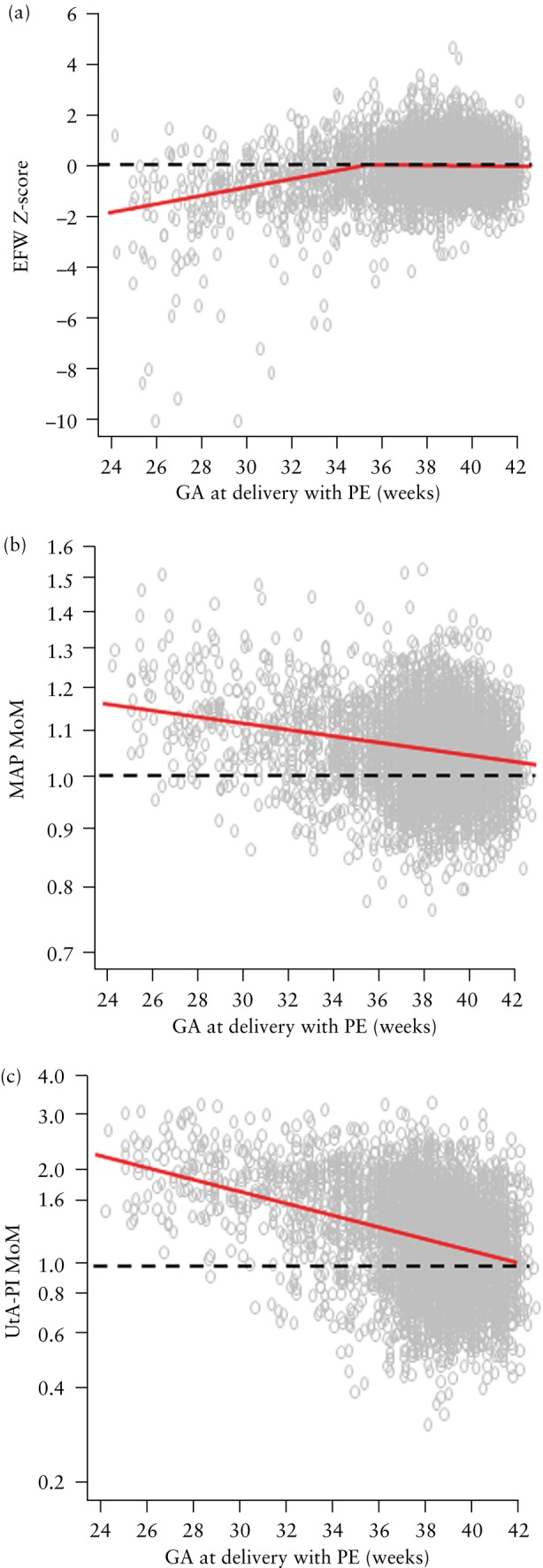
Objective: To stratify pregnancy care based on the estimated risk of pre-eclampsia (PE) from screening at 19-24 weeks' gestation by combinations of maternal risk factors, estimated fetal weight (EFW), mean arterial pressure (MAP) and uterine artery pulsatility index (UtA-PI).
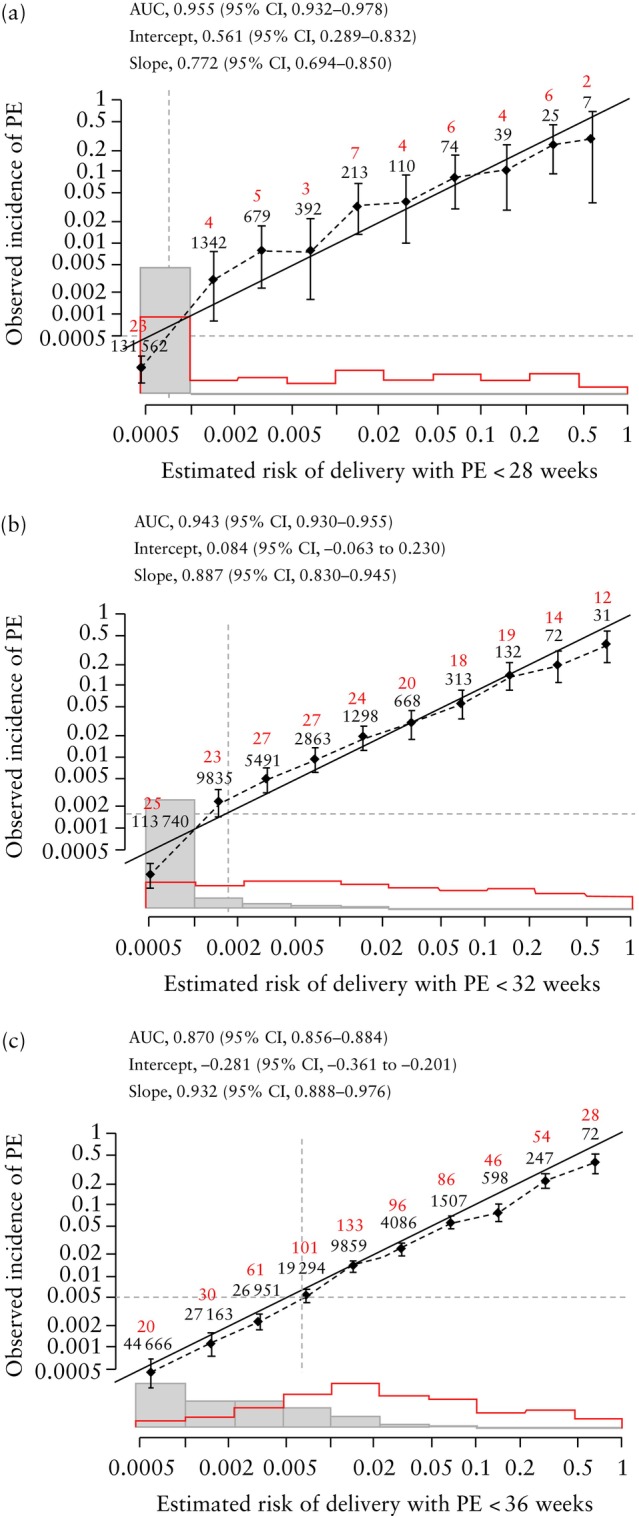
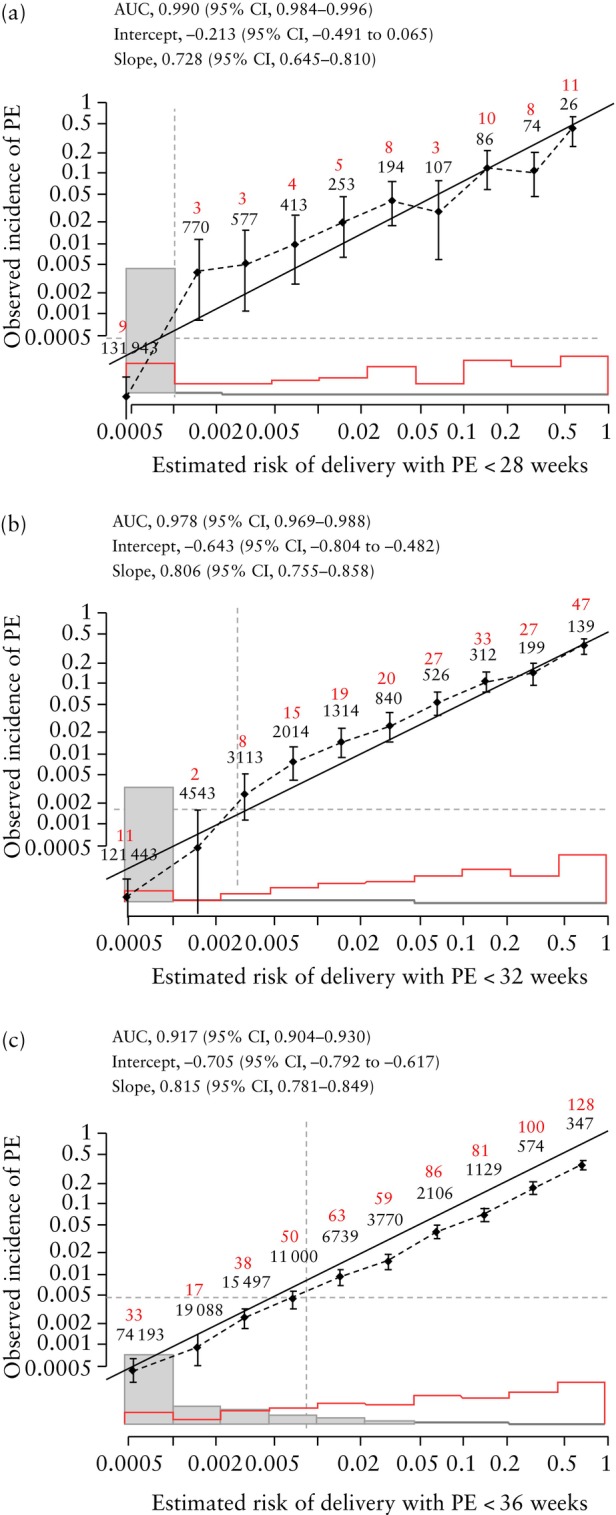
Methods: The data for this study were derived from a prospective non-interventional study in 134 443 women with a singleton pregnancy attending for a routine ultrasound scan at 19 + 0 to 23 + 6 weeks' gestation in two UK maternity hospitals. The visit included recording of maternal demographic characteristics and medical history, sonographic EFW and measurement of MAP and UtA-PI. The competing-risks model was used to estimate the individual patient-specific risk of delivery with PE at < 28, < 32 and < 36 weeks' gestation. Receiver-operating-characteristics curves were constructed for screen-positive rates (SPRs) at different detection rates of delivery with PE at < 28, < 32 and < 36 weeks' gestation for the combinations of maternal risk factors, EFW and MAP, and of maternal risk factors, EFW, MAP and UtA-PI. Different risk cut-offs were used with the intention of detecting about 80%, 85% and 90% of cases of delivery with PE at < 28, < 32 and < 36 weeks' gestation. Calibration for risk of delivery with PE at < 28, < 32 and < 36 weeks' gestation was assessed by plotting the observed incidence of PE against the predicted incidence of PE.
Results: The study population contained 4335 (3.2%) women that subsequently developed PE, including 64 (0.05%) that delivered with PE at < 28 weeks' gestation, 209 (0.2%) that delivered with PE at < 32 weeks and 655 (0.5%) that delivered with PE at < 36 weeks. If the objective of screening was to identify about 90% of cases of delivery with PE at < 28, < 32 and < 36 weeks and the method of screening was a combination of maternal risk factors, EFW and MAP, the respective SPRs would be 11.0%, 18.3% and 38.8%. If the method of screening also included UtA-PI, the respective SPRs would be 2.6%, 3.8% and 23.6%. If the objective of screening was to identify about 80% of cases of delivery with PE at < 28, < 32 and < 36 weeks and the method of screening was a combination of maternal risk factors, EFW and MAP, the respective SPRs would be 5.9%, 9.7% and 21.9%. If the method of screening also included UtA-PI, the respective SPRs would be 1.0%, 2.1% and 11.7%. The calibration plots demonstrated good agreement between the estimated risk and observed incidence of PE.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


