Bertil Kågedal, Anders Helldén, Dženeta Nezirević Dernroth, Anders Lindgaard Andersen, Andreas Ekman, Mats Haglund, Bharti Kataria, Frida Oskarsson, Lovisa Tobieson, Åse Östholm, Håkan Hanberger
{"title":"危重病人对比增强CT后肾小球滤过率的测定:支持一种新方法。","authors":"Bertil Kågedal, Anders Helldén, Dženeta Nezirević Dernroth, Anders Lindgaard Andersen, Andreas Ekman, Mats Haglund, Bharti Kataria, Frida Oskarsson, Lovisa Tobieson, Åse Östholm, Håkan Hanberger","doi":"10.1097/CCE.0000000000001269","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To measure glomerular filtration rate using iohexol plasma clearance (mGFRiohexol) in critically ill patients using the high doses of iohexol administered at CT and to evaluate its agreements with urinary creatinine clearance (uClcr) and estimated glomerular filtration rates (eGFRs), calculated from plasma concentrations of creatinine (eGFRcr) and cystatin C (eGFRcys).</p><p><strong>Design: </strong>Prospective observational cohort study.</p><p><strong>Setting: </strong>ICUs across Southeast Sweden.</p><p><strong>Patients: </strong>Critically ill adult patients.</p><p><strong>Interventions and measurements: </strong>Twenty-six ICU patients were given high doses of iohexol (range, 27-140 mL) for contrast-enhanced CT, whereafter blood samples were taken in the elimination phase for determination of mGFRiohexol. Plasma iohexol concentrations were determined by high-performance liquid chromatography and mGFRiohexol was calculated. Standard dose (5 mL) of iohexol was administered the following days to compare low-dose clearance results with the high-dose clearance results. Six-hour uClcr was performed four times a day and averaged.</p><p><strong>Main results: </strong>Mean ± sd mGFRiohexol after CT was 77.4 ± 38.1 mL/min (n = 26), and uClcr was 97.3 ± 58.2 mL/min (n = 25) in the critically ill patients. There was a strong positive correlation between mGFRiohexol determined with high and low doses of iohexol in patients with normal or high mGFRiohexol (coefficient of determination [R2] = 0.88; p < 0.001) and between mGFRiohexol and uClcr (R2 = 0.87; p < 0.001). eGFRcr overestimated mGFRiohexol and eGFRcys underestimated mGFRiohexol.</p><p><strong>Conclusions: </strong>mGFRiohexol after contrast-enhanced CT compares well with mGFRiohexol after standard low-dose iohexol respectively uClcr. Over- and underestimation of mGFRiohexol by eGFRcr and eGFRcys is probably explained by increased tubular secretion of creatinine and increased production of cystatin C in intensive care patients.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 5","pages":"e1269"},"PeriodicalIF":2.7000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12080682/pdf/","citationCount":"0","resultStr":"{\"title\":\"Determination of Glomerular Filtration Rate After Contrast-Enhanced CT Among Critically Ill Patients: Support for a New Procedure.\",\"authors\":\"Bertil Kågedal, Anders Helldén, Dženeta Nezirević Dernroth, Anders Lindgaard Andersen, Andreas Ekman, Mats Haglund, Bharti Kataria, Frida Oskarsson, Lovisa Tobieson, Åse Östholm, Håkan Hanberger\",\"doi\":\"10.1097/CCE.0000000000001269\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To measure glomerular filtration rate using iohexol plasma clearance (mGFRiohexol) in critically ill patients using the high doses of iohexol administered at CT and to evaluate its agreements with urinary creatinine clearance (uClcr) and estimated glomerular filtration rates (eGFRs), calculated from plasma concentrations of creatinine (eGFRcr) and cystatin C (eGFRcys).</p><p><strong>Design: </strong>Prospective observational cohort study.</p><p><strong>Setting: </strong>ICUs across Southeast Sweden.</p><p><strong>Patients: </strong>Critically ill adult patients.</p><p><strong>Interventions and measurements: </strong>Twenty-six ICU patients were given high doses of iohexol (range, 27-140 mL) for contrast-enhanced CT, whereafter blood samples were taken in the elimination phase for determination of mGFRiohexol. Plasma iohexol concentrations were determined by high-performance liquid chromatography and mGFRiohexol was calculated. Standard dose (5 mL) of iohexol was administered the following days to compare low-dose clearance results with the high-dose clearance results. Six-hour uClcr was performed four times a day and averaged.</p><p><strong>Main results: </strong>Mean ± sd mGFRiohexol after CT was 77.4 ± 38.1 mL/min (n = 26), and uClcr was 97.3 ± 58.2 mL/min (n = 25) in the critically ill patients. There was a strong positive correlation between mGFRiohexol determined with high and low doses of iohexol in patients with normal or high mGFRiohexol (coefficient of determination [R2] = 0.88; p < 0.001) and between mGFRiohexol and uClcr (R2 = 0.87; p < 0.001). eGFRcr overestimated mGFRiohexol and eGFRcys underestimated mGFRiohexol.</p><p><strong>Conclusions: </strong>mGFRiohexol after contrast-enhanced CT compares well with mGFRiohexol after standard low-dose iohexol respectively uClcr. Over- and underestimation of mGFRiohexol by eGFRcr and eGFRcys is probably explained by increased tubular secretion of creatinine and increased production of cystatin C in intensive care patients.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 5\",\"pages\":\"e1269\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12080682/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001269\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001269","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Determination of Glomerular Filtration Rate After Contrast-Enhanced CT Among Critically Ill Patients: Support for a New Procedure.
Objectives: To measure glomerular filtration rate using iohexol plasma clearance (mGFRiohexol) in critically ill patients using the high doses of iohexol administered at CT and to evaluate its agreements with urinary creatinine clearance (uClcr) and estimated glomerular filtration rates (eGFRs), calculated from plasma concentrations of creatinine (eGFRcr) and cystatin C (eGFRcys).
Design: Prospective observational cohort study.
Setting: ICUs across Southeast Sweden.
Patients: Critically ill adult patients.
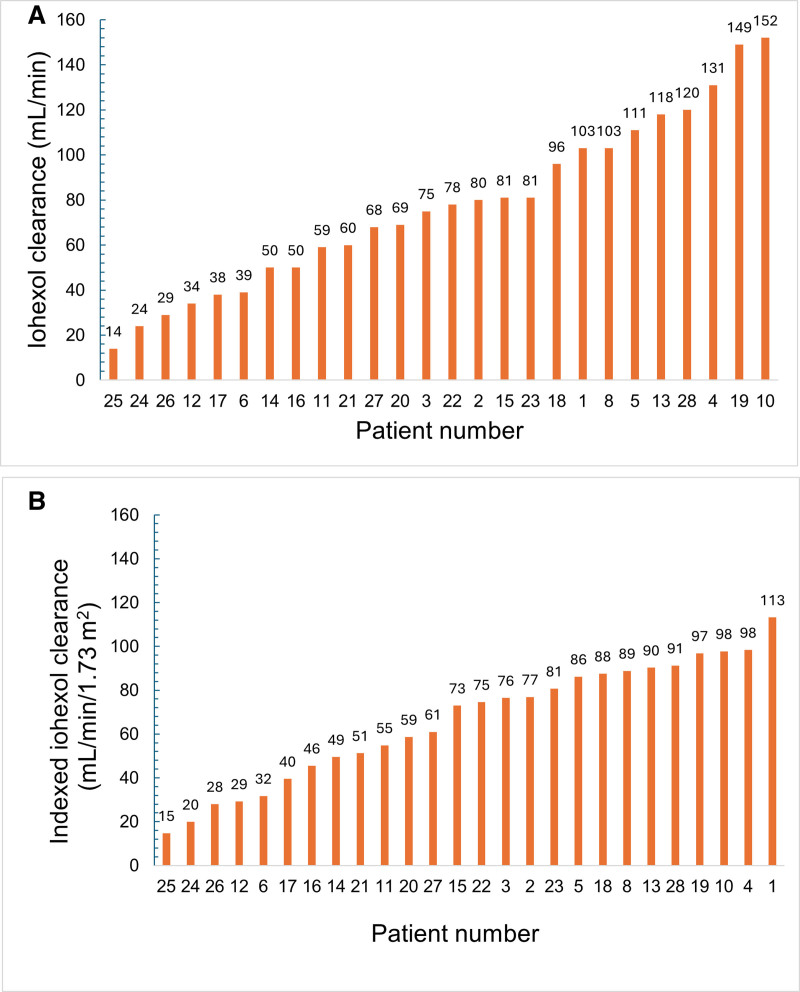
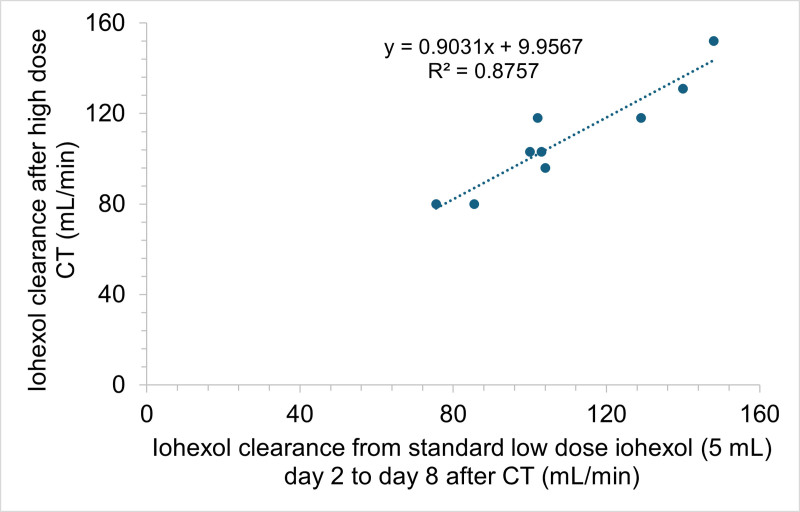
Interventions and measurements: Twenty-six ICU patients were given high doses of iohexol (range, 27-140 mL) for contrast-enhanced CT, whereafter blood samples were taken in the elimination phase for determination of mGFRiohexol. Plasma iohexol concentrations were determined by high-performance liquid chromatography and mGFRiohexol was calculated. Standard dose (5 mL) of iohexol was administered the following days to compare low-dose clearance results with the high-dose clearance results. Six-hour uClcr was performed four times a day and averaged.
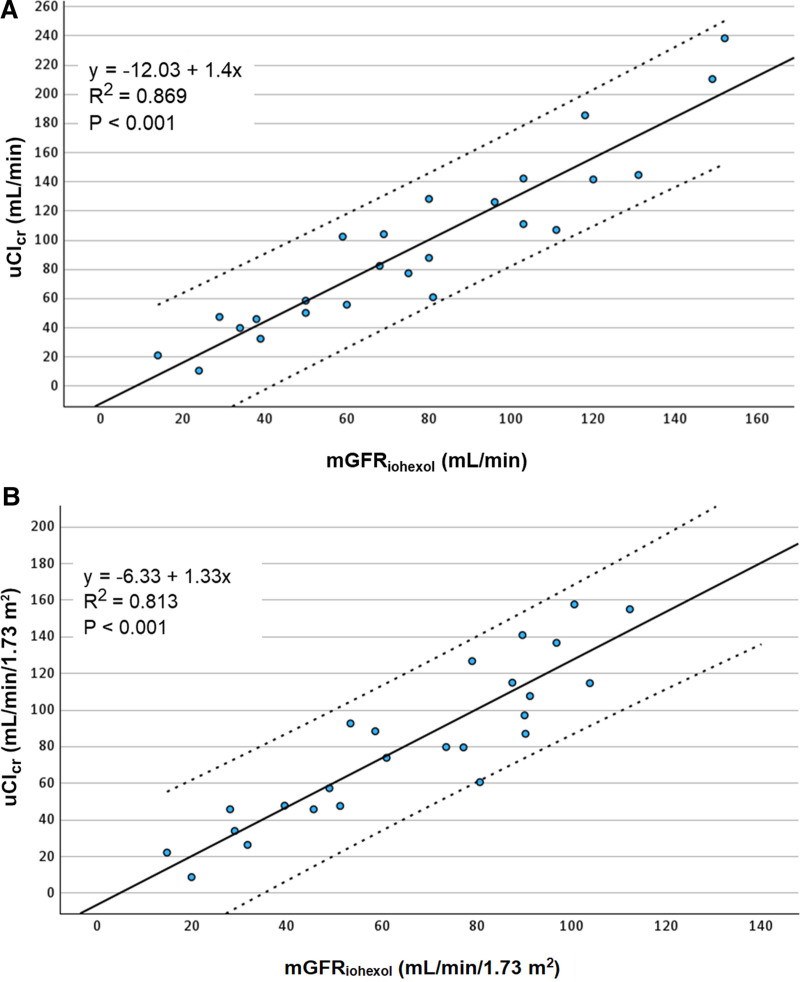
Main results: Mean ± sd mGFRiohexol after CT was 77.4 ± 38.1 mL/min (n = 26), and uClcr was 97.3 ± 58.2 mL/min (n = 25) in the critically ill patients. There was a strong positive correlation between mGFRiohexol determined with high and low doses of iohexol in patients with normal or high mGFRiohexol (coefficient of determination [R2] = 0.88; p < 0.001) and between mGFRiohexol and uClcr (R2 = 0.87; p < 0.001). eGFRcr overestimated mGFRiohexol and eGFRcys underestimated mGFRiohexol.
Conclusions: mGFRiohexol after contrast-enhanced CT compares well with mGFRiohexol after standard low-dose iohexol respectively uClcr. Over- and underestimation of mGFRiohexol by eGFRcr and eGFRcys is probably explained by increased tubular secretion of creatinine and increased production of cystatin C in intensive care patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


