Joseph J Y Wan, Qing H Tan, Dalun Leong, Zhihong Chew, Terry H L Teo
{"title":"机器人导航脊柱手术中髂后上棘参考阵列放置的准确性。","authors":"Joseph J Y Wan, Qing H Tan, Dalun Leong, Zhihong Chew, Terry H L Teo","doi":"10.1302/2633-1462.65.BJO-2025-0006.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Computer-navigated spinal instrumentation requires placement of a dynamic reference base (DRB), typically intraosseously in the ilium via a percutaneous stab incision on the posterior superior iliac spine (PSIS) entry point. Data describing the accuracy and complications of DRB placement are limited in the literature. The aim of this study is to measure the accuracy of DRB placement in the PSIS, determine its exact placement trajectory, and determine the prevalence of related complications.</p><p><strong>Methods: </strong>This is a single-centre, institutional board approved, multisurgeon retrospective analysis of 69 included DRB placements from 51 robot-assisted lumbar posterior instrumentation procedures between May 2022 and April 2024. Pin entry point and trajectory were mapped out; the intraoperative O-arm CT scans and skin-to-PSIS depth were also measured, and patient demographics (age, sex, BMI), surgical outcomes, and postoperative complications were recorded.</p><p><strong>Results: </strong>Of the 69 PSIS pin placements, 47 (68.1%) had the correct entry point on the PSIS, and 35 (50.7%) of them were placed correctly within the ilium without breaching a second cortex. Skin-to-PSIS depth was significantly higher in patients with misplaced DRB placement, while age, sex, and BMI were similar. Of those with misplaced DRB (n = 34), one had delayed pin site wound healing.</p><p><strong>Conclusion: </strong>Percutaneous PSIS DRB placement has poor accuracy, with skin-to-PSIS depth being a significant factor. To avoid complications from misplaced DRB placement, the authors recommend the use of DRB placement on the iliac wing, or on the PSIS, following the trajectory used in pelvis posterior column fracture fixation, using fluoroscopy intraoperatively to ensure the DRB pin position.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 5","pages":"528-534"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12045663/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of posterosuperior iliac spine reference array placement in robot-navigated spine surgery.\",\"authors\":\"Joseph J Y Wan, Qing H Tan, Dalun Leong, Zhihong Chew, Terry H L Teo\",\"doi\":\"10.1302/2633-1462.65.BJO-2025-0006.R1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Computer-navigated spinal instrumentation requires placement of a dynamic reference base (DRB), typically intraosseously in the ilium via a percutaneous stab incision on the posterior superior iliac spine (PSIS) entry point. Data describing the accuracy and complications of DRB placement are limited in the literature. The aim of this study is to measure the accuracy of DRB placement in the PSIS, determine its exact placement trajectory, and determine the prevalence of related complications.</p><p><strong>Methods: </strong>This is a single-centre, institutional board approved, multisurgeon retrospective analysis of 69 included DRB placements from 51 robot-assisted lumbar posterior instrumentation procedures between May 2022 and April 2024. Pin entry point and trajectory were mapped out; the intraoperative O-arm CT scans and skin-to-PSIS depth were also measured, and patient demographics (age, sex, BMI), surgical outcomes, and postoperative complications were recorded.</p><p><strong>Results: </strong>Of the 69 PSIS pin placements, 47 (68.1%) had the correct entry point on the PSIS, and 35 (50.7%) of them were placed correctly within the ilium without breaching a second cortex. Skin-to-PSIS depth was significantly higher in patients with misplaced DRB placement, while age, sex, and BMI were similar. Of those with misplaced DRB (n = 34), one had delayed pin site wound healing.</p><p><strong>Conclusion: </strong>Percutaneous PSIS DRB placement has poor accuracy, with skin-to-PSIS depth being a significant factor. To avoid complications from misplaced DRB placement, the authors recommend the use of DRB placement on the iliac wing, or on the PSIS, following the trajectory used in pelvis posterior column fracture fixation, using fluoroscopy intraoperatively to ensure the DRB pin position.</p>\",\"PeriodicalId\":34103,\"journal\":{\"name\":\"Bone & Joint Open\",\"volume\":\"6 5\",\"pages\":\"528-534\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12045663/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bone & Joint Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1302/2633-1462.65.BJO-2025-0006.R1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.65.BJO-2025-0006.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Accuracy of posterosuperior iliac spine reference array placement in robot-navigated spine surgery.
Aims: Computer-navigated spinal instrumentation requires placement of a dynamic reference base (DRB), typically intraosseously in the ilium via a percutaneous stab incision on the posterior superior iliac spine (PSIS) entry point. Data describing the accuracy and complications of DRB placement are limited in the literature. The aim of this study is to measure the accuracy of DRB placement in the PSIS, determine its exact placement trajectory, and determine the prevalence of related complications.
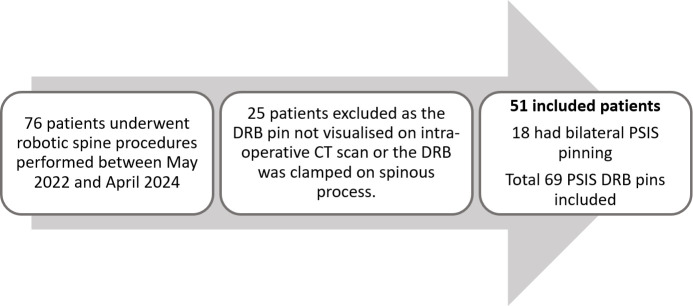
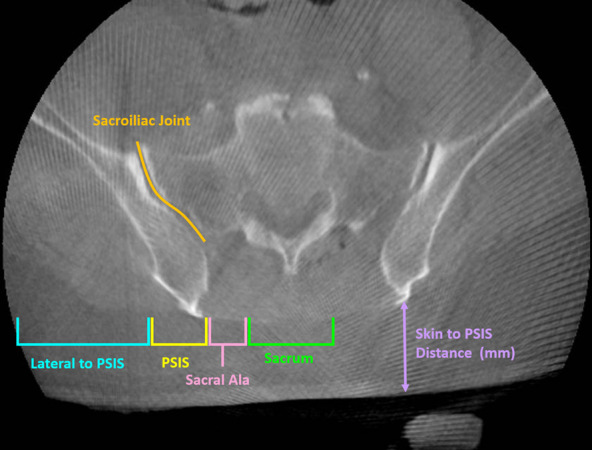
Methods: This is a single-centre, institutional board approved, multisurgeon retrospective analysis of 69 included DRB placements from 51 robot-assisted lumbar posterior instrumentation procedures between May 2022 and April 2024. Pin entry point and trajectory were mapped out; the intraoperative O-arm CT scans and skin-to-PSIS depth were also measured, and patient demographics (age, sex, BMI), surgical outcomes, and postoperative complications were recorded.
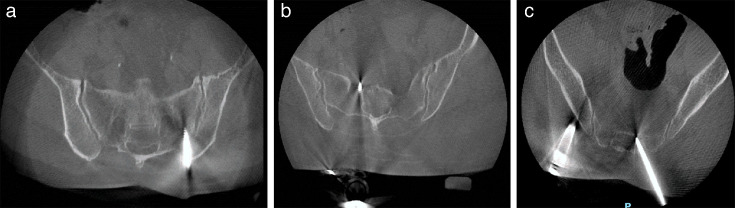
Results: Of the 69 PSIS pin placements, 47 (68.1%) had the correct entry point on the PSIS, and 35 (50.7%) of them were placed correctly within the ilium without breaching a second cortex. Skin-to-PSIS depth was significantly higher in patients with misplaced DRB placement, while age, sex, and BMI were similar. Of those with misplaced DRB (n = 34), one had delayed pin site wound healing.
Conclusion: Percutaneous PSIS DRB placement has poor accuracy, with skin-to-PSIS depth being a significant factor. To avoid complications from misplaced DRB placement, the authors recommend the use of DRB placement on the iliac wing, or on the PSIS, following the trajectory used in pelvis posterior column fracture fixation, using fluoroscopy intraoperatively to ensure the DRB pin position.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


