Murilo Tavares Valverde Filho, Gabriel Vianna Pereira Aragão, Igor Lima Vieira de Castro, Jade de Oliveira Santana, Liana Codes, Claudio Celestino Zollinger, Wellington Andraus, Paulo Lisboa Bittencourt
{"title":"择期和急诊剖腹手术后入住重症监护病房的患者的术后预后。","authors":"Murilo Tavares Valverde Filho, Gabriel Vianna Pereira Aragão, Igor Lima Vieira de Castro, Jade de Oliveira Santana, Liana Codes, Claudio Celestino Zollinger, Wellington Andraus, Paulo Lisboa Bittencourt","doi":"10.1590/0102-67202025000010e1879","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgery is associated with a high risk for morbidity and mortality, particularly when performed in critical patients requiring intensive care unit (ICU) admission.</p><p><strong>Aim: </strong>The aim of this study was to investigate risk factors associated with adverse outcomes in a large cohort of patients admitted to a single-center ICU after abdominal surgery.</p><p><strong>Methods: </strong>All patients admitted to a surgical ICU for postoperative care, from January 2016 to December 2022, were retrospectively evaluated. Data concerning demographics and clinical and perioperative variables were compared to in-hospital mortality.</p><p><strong>Results: </strong>A total of 1,717 patients (1,096 women, mean age: 61±17 years) were evaluated. Most of the patients underwent colorectal (n=499), pancreatic (n=148), biliary tract (n=147), and gastric surgeries (n=145); liver resection (n=131); and several gynecological or obstetric procedures (n=250). Only 52.3% of these surgical procedures were elective. The mean Charlson Comorbidity Index (CCI) and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were 4.4±2.8 and 10.1±5.6, respectively. Mortality was observed in 158 (9.2%) patients. Age (70.4±14.3 vs. 60.6±17.1 years in survivors, p=0.002), CCI (6.1±2.5 vs. 4.3±2.8 in survivors, p=0.005), type of surgery (13.6% in emergent/urgent vs. 5.5% in elective surgeries, p<0.001), and APACHE II score (16.7±8.4 vs. 9.4±4.7 in survivors, p<0.0001) were associated with mortality on univariate analysis, but only CCI, type of surgery, and APACHE II score were independently correlated with a higher risk of death on multivariate analysis.</p><p><strong>Conclusions: </strong>Mortality after abdominal surgery in patients requiring postoperative ICU support is less than 10% nowadays, and it is independently associated with urgent or emergent surgeries, disease severity, and comorbidity.</p>","PeriodicalId":72298,"journal":{"name":"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery","volume":"38 ","pages":"e1879"},"PeriodicalIF":1.8000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12023906/pdf/","citationCount":"0","resultStr":"{\"title\":\"POSTOPERATIVE OUTCOME OF PATIENTS ADMITTED TO THE INTENSIVE CARE UNIT AFTER ELECTIVE AND EMERGENCY LAPAROTOMY.\",\"authors\":\"Murilo Tavares Valverde Filho, Gabriel Vianna Pereira Aragão, Igor Lima Vieira de Castro, Jade de Oliveira Santana, Liana Codes, Claudio Celestino Zollinger, Wellington Andraus, Paulo Lisboa Bittencourt\",\"doi\":\"10.1590/0102-67202025000010e1879\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Surgery is associated with a high risk for morbidity and mortality, particularly when performed in critical patients requiring intensive care unit (ICU) admission.</p><p><strong>Aim: </strong>The aim of this study was to investigate risk factors associated with adverse outcomes in a large cohort of patients admitted to a single-center ICU after abdominal surgery.</p><p><strong>Methods: </strong>All patients admitted to a surgical ICU for postoperative care, from January 2016 to December 2022, were retrospectively evaluated. Data concerning demographics and clinical and perioperative variables were compared to in-hospital mortality.</p><p><strong>Results: </strong>A total of 1,717 patients (1,096 women, mean age: 61±17 years) were evaluated. Most of the patients underwent colorectal (n=499), pancreatic (n=148), biliary tract (n=147), and gastric surgeries (n=145); liver resection (n=131); and several gynecological or obstetric procedures (n=250). Only 52.3% of these surgical procedures were elective. The mean Charlson Comorbidity Index (CCI) and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were 4.4±2.8 and 10.1±5.6, respectively. Mortality was observed in 158 (9.2%) patients. Age (70.4±14.3 vs. 60.6±17.1 years in survivors, p=0.002), CCI (6.1±2.5 vs. 4.3±2.8 in survivors, p=0.005), type of surgery (13.6% in emergent/urgent vs. 5.5% in elective surgeries, p<0.001), and APACHE II score (16.7±8.4 vs. 9.4±4.7 in survivors, p<0.0001) were associated with mortality on univariate analysis, but only CCI, type of surgery, and APACHE II score were independently correlated with a higher risk of death on multivariate analysis.</p><p><strong>Conclusions: </strong>Mortality after abdominal surgery in patients requiring postoperative ICU support is less than 10% nowadays, and it is independently associated with urgent or emergent surgeries, disease severity, and comorbidity.</p>\",\"PeriodicalId\":72298,\"journal\":{\"name\":\"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery\",\"volume\":\"38 \",\"pages\":\"e1879\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12023906/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1590/0102-67202025000010e1879\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1590/0102-67202025000010e1879","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
POSTOPERATIVE OUTCOME OF PATIENTS ADMITTED TO THE INTENSIVE CARE UNIT AFTER ELECTIVE AND EMERGENCY LAPAROTOMY.
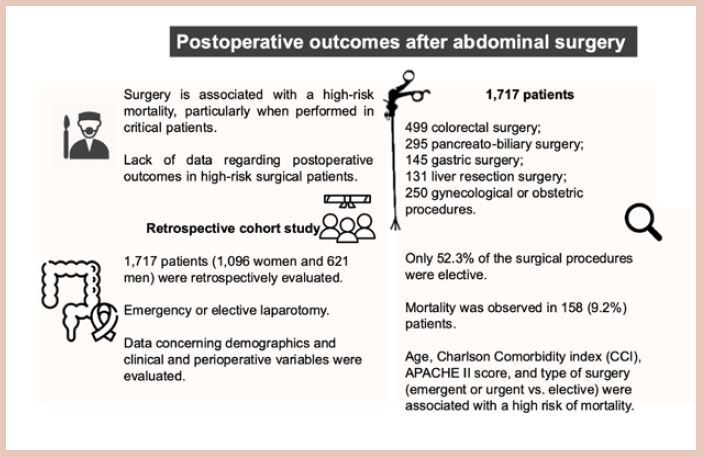
Background: Surgery is associated with a high risk for morbidity and mortality, particularly when performed in critical patients requiring intensive care unit (ICU) admission.
Aim: The aim of this study was to investigate risk factors associated with adverse outcomes in a large cohort of patients admitted to a single-center ICU after abdominal surgery.
Methods: All patients admitted to a surgical ICU for postoperative care, from January 2016 to December 2022, were retrospectively evaluated. Data concerning demographics and clinical and perioperative variables were compared to in-hospital mortality.
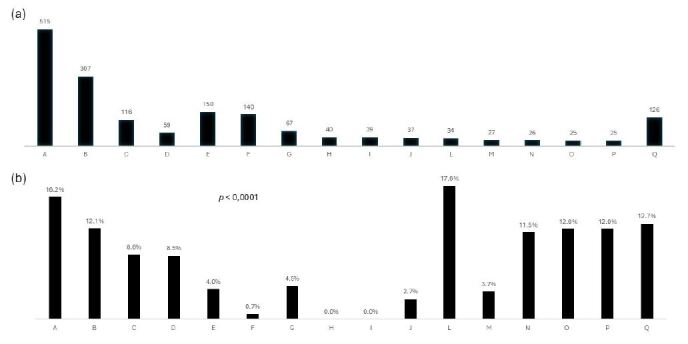
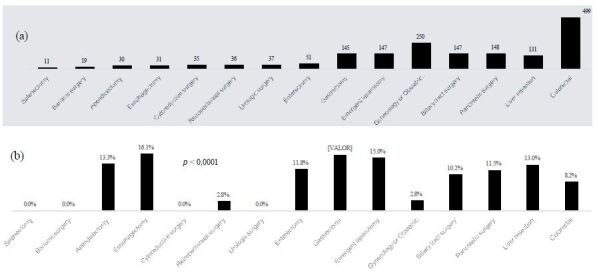
Results: A total of 1,717 patients (1,096 women, mean age: 61±17 years) were evaluated. Most of the patients underwent colorectal (n=499), pancreatic (n=148), biliary tract (n=147), and gastric surgeries (n=145); liver resection (n=131); and several gynecological or obstetric procedures (n=250). Only 52.3% of these surgical procedures were elective. The mean Charlson Comorbidity Index (CCI) and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were 4.4±2.8 and 10.1±5.6, respectively. Mortality was observed in 158 (9.2%) patients. Age (70.4±14.3 vs. 60.6±17.1 years in survivors, p=0.002), CCI (6.1±2.5 vs. 4.3±2.8 in survivors, p=0.005), type of surgery (13.6% in emergent/urgent vs. 5.5% in elective surgeries, p<0.001), and APACHE II score (16.7±8.4 vs. 9.4±4.7 in survivors, p<0.0001) were associated with mortality on univariate analysis, but only CCI, type of surgery, and APACHE II score were independently correlated with a higher risk of death on multivariate analysis.
Conclusions: Mortality after abdominal surgery in patients requiring postoperative ICU support is less than 10% nowadays, and it is independently associated with urgent or emergent surgeries, disease severity, and comorbidity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


