David Z Rose, Alejandro A Rabinstein, May Kim-Tenser, Sergio D Bergese, Gabriel V Fontaine, Charles Kircher, Adnan I Qureshi
{"title":"急性缺血性脑卒中和脑出血后血压变异性:定义、干预机会和研究方向","authors":"David Z Rose, Alejandro A Rabinstein, May Kim-Tenser, Sergio D Bergese, Gabriel V Fontaine, Charles Kircher, Adnan I Qureshi","doi":"10.1007/s12028-025-02263-8","DOIUrl":null,"url":null,"abstract":"<p><p>Increased blood pressure variability (BPV) in the acute phases of cerebrovascular emergencies, such as acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH), has been shown to result in worsened outcomes. Although several studies have reported this association, no consensus exists for specific BPV targets or a consistent, unified definition of BPV in AIS or ICH. Therefore, we convened the Blood Pressure Variability in Cerebrovascular Emergencies Consortia, consisting of a multidisciplinary group of experts in stroke, neurocritical care, perioperative medicine, emergency medicine, and clinical pharmacy to assess the clinical impact of BPV and to develop a working consensus on defining BPV, identifying interventions to mitigate negative outcomes from increased BPV, and laying the groundwork for BPV research concepts in the future. First, the Consortia proposed bifurcating systolic BPV (SBPV) into two distinct periods-SBPV<sub>1</sub> and SBPV<sub>2</sub>. SBPV<sub>1</sub> involves hyperacute management, when rapid and smooth blood pressure control is crucial. SBPV<sub>2</sub>, the plateauing phase, consists of a more gradual, maintenance-therapy slope. For both periods, enabling a \"smooth\" (SBPV<sub>1</sub>) and \"sustained\" (SBPV<sub>2</sub>) trajectory is likely ideal, but more phase-specific research is required to validate this concept. Secondly, Consortia proposed to calculate BPV by subtracting maximum and minimum systolic blood pressure over subsequent measurements because it represents the most clinically feasible option among many proposed equations in the literature. Third, for ICH, the Consortia preferred intravenous antihypertensive medication to reach BPV goals as fast, safe, and efficiently as possible, consistent with American Heart Association/American Stroke Association guidelines recommending \"treatment regimens that limit BPV and achieve smooth, sustained blood pressure control.\" For AIS, guidelines do not yet address BPV, but Consortia members proposed an algorithm with distinct SBPV goals based on time (as a function of stroke acuity), arterial subtype (large, medium, and small vessel), thrombolytic and/or thrombectomy status, and presenting SBP. As the understanding of BPV evolves, future research may build on and/or refine concepts proposed by this Consortia.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"368-377"},"PeriodicalIF":3.6000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436555/pdf/","citationCount":"0","resultStr":"{\"title\":\"Blood Pressure Variability After Acute Ischemic Stroke and Intracerebral Hemorrhage: Refining Its Definition, Intervention Opportunities, and Research Directions.\",\"authors\":\"David Z Rose, Alejandro A Rabinstein, May Kim-Tenser, Sergio D Bergese, Gabriel V Fontaine, Charles Kircher, Adnan I Qureshi\",\"doi\":\"10.1007/s12028-025-02263-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Increased blood pressure variability (BPV) in the acute phases of cerebrovascular emergencies, such as acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH), has been shown to result in worsened outcomes. Although several studies have reported this association, no consensus exists for specific BPV targets or a consistent, unified definition of BPV in AIS or ICH. Therefore, we convened the Blood Pressure Variability in Cerebrovascular Emergencies Consortia, consisting of a multidisciplinary group of experts in stroke, neurocritical care, perioperative medicine, emergency medicine, and clinical pharmacy to assess the clinical impact of BPV and to develop a working consensus on defining BPV, identifying interventions to mitigate negative outcomes from increased BPV, and laying the groundwork for BPV research concepts in the future. First, the Consortia proposed bifurcating systolic BPV (SBPV) into two distinct periods-SBPV<sub>1</sub> and SBPV<sub>2</sub>. SBPV<sub>1</sub> involves hyperacute management, when rapid and smooth blood pressure control is crucial. SBPV<sub>2</sub>, the plateauing phase, consists of a more gradual, maintenance-therapy slope. For both periods, enabling a \\\"smooth\\\" (SBPV<sub>1</sub>) and \\\"sustained\\\" (SBPV<sub>2</sub>) trajectory is likely ideal, but more phase-specific research is required to validate this concept. Secondly, Consortia proposed to calculate BPV by subtracting maximum and minimum systolic blood pressure over subsequent measurements because it represents the most clinically feasible option among many proposed equations in the literature. Third, for ICH, the Consortia preferred intravenous antihypertensive medication to reach BPV goals as fast, safe, and efficiently as possible, consistent with American Heart Association/American Stroke Association guidelines recommending \\\"treatment regimens that limit BPV and achieve smooth, sustained blood pressure control.\\\" For AIS, guidelines do not yet address BPV, but Consortia members proposed an algorithm with distinct SBPV goals based on time (as a function of stroke acuity), arterial subtype (large, medium, and small vessel), thrombolytic and/or thrombectomy status, and presenting SBP. As the understanding of BPV evolves, future research may build on and/or refine concepts proposed by this Consortia.</p>\",\"PeriodicalId\":19118,\"journal\":{\"name\":\"Neurocritical Care\",\"volume\":\" \",\"pages\":\"368-377\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436555/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurocritical Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12028-025-02263-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-025-02263-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Blood Pressure Variability After Acute Ischemic Stroke and Intracerebral Hemorrhage: Refining Its Definition, Intervention Opportunities, and Research Directions.
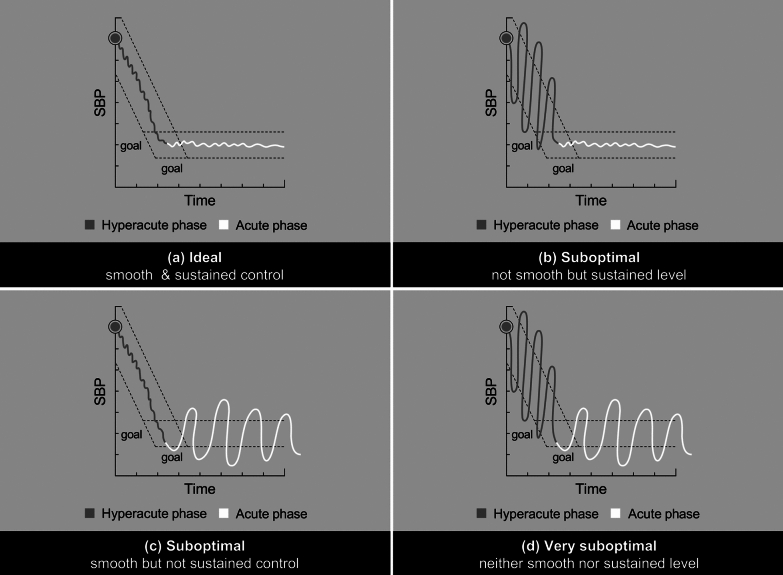
Increased blood pressure variability (BPV) in the acute phases of cerebrovascular emergencies, such as acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH), has been shown to result in worsened outcomes. Although several studies have reported this association, no consensus exists for specific BPV targets or a consistent, unified definition of BPV in AIS or ICH. Therefore, we convened the Blood Pressure Variability in Cerebrovascular Emergencies Consortia, consisting of a multidisciplinary group of experts in stroke, neurocritical care, perioperative medicine, emergency medicine, and clinical pharmacy to assess the clinical impact of BPV and to develop a working consensus on defining BPV, identifying interventions to mitigate negative outcomes from increased BPV, and laying the groundwork for BPV research concepts in the future. First, the Consortia proposed bifurcating systolic BPV (SBPV) into two distinct periods-SBPV1 and SBPV2. SBPV1 involves hyperacute management, when rapid and smooth blood pressure control is crucial. SBPV2, the plateauing phase, consists of a more gradual, maintenance-therapy slope. For both periods, enabling a "smooth" (SBPV1) and "sustained" (SBPV2) trajectory is likely ideal, but more phase-specific research is required to validate this concept. Secondly, Consortia proposed to calculate BPV by subtracting maximum and minimum systolic blood pressure over subsequent measurements because it represents the most clinically feasible option among many proposed equations in the literature. Third, for ICH, the Consortia preferred intravenous antihypertensive medication to reach BPV goals as fast, safe, and efficiently as possible, consistent with American Heart Association/American Stroke Association guidelines recommending "treatment regimens that limit BPV and achieve smooth, sustained blood pressure control." For AIS, guidelines do not yet address BPV, but Consortia members proposed an algorithm with distinct SBPV goals based on time (as a function of stroke acuity), arterial subtype (large, medium, and small vessel), thrombolytic and/or thrombectomy status, and presenting SBP. As the understanding of BPV evolves, future research may build on and/or refine concepts proposed by this Consortia.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


