Satoru Mitsuboshi, Shungo Imai, Masami Tsuchiya, Hayato Kizaki, Satoko Hori
{"title":"日本急性肾损伤诊断编码的准确性——基于日本医院数据库的分析","authors":"Satoru Mitsuboshi, Shungo Imai, Masami Tsuchiya, Hayato Kizaki, Satoko Hori","doi":"10.1002/pds.70146","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To evaluate the accuracy of diagnostic coding for acute kidney injury (AKI) in Japan.</p><p><strong>Methods: </strong>The data analyzed were obtained from the JMDC hospital-based administrative claims database from cases registered between April 2014 and August 2022. Only patients who underwent serum creatinine measurements two or more times with intervals of 7 days or less were eligible for inclusion. AKIs were identified by International Classification of Diseases 10th Revision (ICD-10) codes N14 and N17. These were assessed according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria.</p><p><strong>Results: </strong>A total of 467 019 patients (median age, 74 [range, 20-99] years; male, 50.9%) were eligible for inclusion. Among these patients, 1849 (0.4%) were assigned ICD-10 codes for AKI. Among these 1849 patients, the code was assigned within 7 days of the occurrence of AKI (as defined by the KDIGO criteria) in 212 patients, within 14 days in 294 patients, and within 30 days in 386 patients. The positive predictive values and 95% confidence intervals of the ICD-10 code for AKI at these timepoints were as follows: within 7 days, 11.5% (10.1%-13.0%); within 14 days, 15.9% (14.3%-17.6%); and within 30 days, 20.9% (19.1%-22.8%).</p><p><strong>Conclusions: </strong>The ICD-10 codes for AKI showed poor positive predictive values for AKI as defined by the KDIGO criteria, suggesting that it may be difficult to identify AKI using ICD-10 codes alone in the Japanese context.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 4","pages":"e70146"},"PeriodicalIF":2.4000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11987052/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of Diagnostic Coding for Acute Kidney Injury in Japan-Analysis of a Japanese Hospital-Based Database.\",\"authors\":\"Satoru Mitsuboshi, Shungo Imai, Masami Tsuchiya, Hayato Kizaki, Satoko Hori\",\"doi\":\"10.1002/pds.70146\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To evaluate the accuracy of diagnostic coding for acute kidney injury (AKI) in Japan.</p><p><strong>Methods: </strong>The data analyzed were obtained from the JMDC hospital-based administrative claims database from cases registered between April 2014 and August 2022. Only patients who underwent serum creatinine measurements two or more times with intervals of 7 days or less were eligible for inclusion. AKIs were identified by International Classification of Diseases 10th Revision (ICD-10) codes N14 and N17. These were assessed according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria.</p><p><strong>Results: </strong>A total of 467 019 patients (median age, 74 [range, 20-99] years; male, 50.9%) were eligible for inclusion. Among these patients, 1849 (0.4%) were assigned ICD-10 codes for AKI. Among these 1849 patients, the code was assigned within 7 days of the occurrence of AKI (as defined by the KDIGO criteria) in 212 patients, within 14 days in 294 patients, and within 30 days in 386 patients. The positive predictive values and 95% confidence intervals of the ICD-10 code for AKI at these timepoints were as follows: within 7 days, 11.5% (10.1%-13.0%); within 14 days, 15.9% (14.3%-17.6%); and within 30 days, 20.9% (19.1%-22.8%).</p><p><strong>Conclusions: </strong>The ICD-10 codes for AKI showed poor positive predictive values for AKI as defined by the KDIGO criteria, suggesting that it may be difficult to identify AKI using ICD-10 codes alone in the Japanese context.</p>\",\"PeriodicalId\":19782,\"journal\":{\"name\":\"Pharmacoepidemiology and Drug Safety\",\"volume\":\"34 4\",\"pages\":\"e70146\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11987052/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pharmacoepidemiology and Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/pds.70146\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70146","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Accuracy of Diagnostic Coding for Acute Kidney Injury in Japan-Analysis of a Japanese Hospital-Based Database.
Purpose: To evaluate the accuracy of diagnostic coding for acute kidney injury (AKI) in Japan.
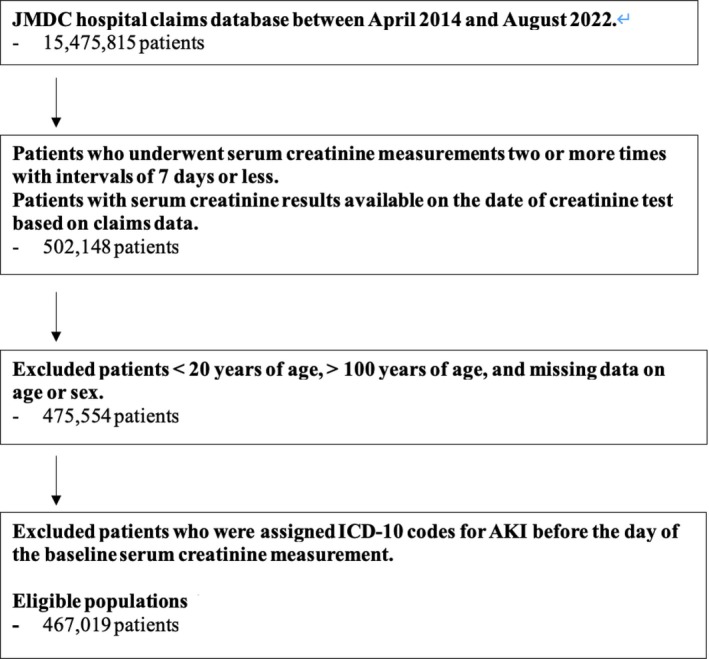
Methods: The data analyzed were obtained from the JMDC hospital-based administrative claims database from cases registered between April 2014 and August 2022. Only patients who underwent serum creatinine measurements two or more times with intervals of 7 days or less were eligible for inclusion. AKIs were identified by International Classification of Diseases 10th Revision (ICD-10) codes N14 and N17. These were assessed according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria.
Results: A total of 467 019 patients (median age, 74 [range, 20-99] years; male, 50.9%) were eligible for inclusion. Among these patients, 1849 (0.4%) were assigned ICD-10 codes for AKI. Among these 1849 patients, the code was assigned within 7 days of the occurrence of AKI (as defined by the KDIGO criteria) in 212 patients, within 14 days in 294 patients, and within 30 days in 386 patients. The positive predictive values and 95% confidence intervals of the ICD-10 code for AKI at these timepoints were as follows: within 7 days, 11.5% (10.1%-13.0%); within 14 days, 15.9% (14.3%-17.6%); and within 30 days, 20.9% (19.1%-22.8%).
Conclusions: The ICD-10 codes for AKI showed poor positive predictive values for AKI as defined by the KDIGO criteria, suggesting that it may be difficult to identify AKI using ICD-10 codes alone in the Japanese context.
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


