Murilo Bacchini Dias, Thiago J. Avelino-Silva, Eduardo Ferriolli, Leandro Utino Taniguchi, Wilson Jacob-Filho, Claudia Kimie Suemoto, Márlon Juliano Romero Aliberti, the CO-FRAIL Study Group for the COVID HCFMUSP Study Group
{"title":"出院后COVID-19症状预测1年功能下降、跌倒和急诊就诊:一项队列研究","authors":"Murilo Bacchini Dias, Thiago J. Avelino-Silva, Eduardo Ferriolli, Leandro Utino Taniguchi, Wilson Jacob-Filho, Claudia Kimie Suemoto, Márlon Juliano Romero Aliberti, the CO-FRAIL Study Group for the COVID HCFMUSP Study Group","doi":"10.1111/jgs.19490","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Hospitalization frequently results in persistent symptoms among older adults, raising concerns about the long-term impacts of acute events—a problem amplified by COVID-19. We investigated the effects of persistent symptoms on functional decline and unplanned events over 1 year in older patients recovering from COVID-19 hospitalization.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This prospective cohort included patients aged ≥ 50 years who survived COVID-19 hospitalization between March and December 2020 as part of the CO-FRAIL study at Brazil's largest academic medical center. Persistent symptoms were defined as those reported at admission and continuously present at one-, three-, six-, nine-, and 12-month post-discharge, covering 16 symptoms. Outcomes included functional decline in basic activities of daily living (ADL), mobility activities, instrumental activities of daily living (IADL), number of falls, emergency department (ED) visits, and hospital readmissions. Associations between persistent symptoms and outcomes were examined using mixed-effects negative binomial regression models adjusted for sociodemographic, clinical, hospitalization-related factors, and post-discharge rehabilitation.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Among 1019 patients (mean age = 65 ± 10 years; women = 45%; White = 62%), 324 (32%) experienced persistent symptoms throughout the year. Fatigue (28%), myalgia (19%), and dyspnea (13%) were the most common. Patients with ≥ 2 symptoms had an increased risk of functional decline in mobility activities (IRR = 2.11; 95% CI = 1.50–2.96), IADL (IRR = 2.00; 95% CI = 1.44–2.79), falls (IRR = 2.56; 95% CI = 1.14–5.75), and ED visits (IRR = 2.69; 95% CI = 1.27–5.70), but not readmissions. Among women, ≥ 1 persistent symptom was associated with a twofold increased risk of ADL decline. One year after discharge, patients with ≥ 2 persistent symptoms developed 1.27 more new disabilities (3.26 vs. 1.99 on a 15-point functional scale) and had 31 more unplanned events per 100 person-years (54.3 vs. 23.2) than those without symptoms.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Persistent symptoms after hospitalization are common and contribute to functional decline, falls, and ED visits in older COVID-19 survivors. These findings suggest that greater attention to symptom burden may support risk identification and improve post-discharge care planning.</p>\n </section>\n </div>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"73 6","pages":"1722-1732"},"PeriodicalIF":4.5000,"publicationDate":"2025-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19490","citationCount":"0","resultStr":"{\"title\":\"Post-Discharge COVID-19 Symptoms Predict 1-Year Functional Decline, Falls, and Emergency Department Visits: A Cohort Study\",\"authors\":\"Murilo Bacchini Dias, Thiago J. Avelino-Silva, Eduardo Ferriolli, Leandro Utino Taniguchi, Wilson Jacob-Filho, Claudia Kimie Suemoto, Márlon Juliano Romero Aliberti, the CO-FRAIL Study Group for the COVID HCFMUSP Study Group\",\"doi\":\"10.1111/jgs.19490\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Hospitalization frequently results in persistent symptoms among older adults, raising concerns about the long-term impacts of acute events—a problem amplified by COVID-19. We investigated the effects of persistent symptoms on functional decline and unplanned events over 1 year in older patients recovering from COVID-19 hospitalization.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This prospective cohort included patients aged ≥ 50 years who survived COVID-19 hospitalization between March and December 2020 as part of the CO-FRAIL study at Brazil's largest academic medical center. Persistent symptoms were defined as those reported at admission and continuously present at one-, three-, six-, nine-, and 12-month post-discharge, covering 16 symptoms. Outcomes included functional decline in basic activities of daily living (ADL), mobility activities, instrumental activities of daily living (IADL), number of falls, emergency department (ED) visits, and hospital readmissions. Associations between persistent symptoms and outcomes were examined using mixed-effects negative binomial regression models adjusted for sociodemographic, clinical, hospitalization-related factors, and post-discharge rehabilitation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Among 1019 patients (mean age = 65 ± 10 years; women = 45%; White = 62%), 324 (32%) experienced persistent symptoms throughout the year. Fatigue (28%), myalgia (19%), and dyspnea (13%) were the most common. Patients with ≥ 2 symptoms had an increased risk of functional decline in mobility activities (IRR = 2.11; 95% CI = 1.50–2.96), IADL (IRR = 2.00; 95% CI = 1.44–2.79), falls (IRR = 2.56; 95% CI = 1.14–5.75), and ED visits (IRR = 2.69; 95% CI = 1.27–5.70), but not readmissions. Among women, ≥ 1 persistent symptom was associated with a twofold increased risk of ADL decline. One year after discharge, patients with ≥ 2 persistent symptoms developed 1.27 more new disabilities (3.26 vs. 1.99 on a 15-point functional scale) and had 31 more unplanned events per 100 person-years (54.3 vs. 23.2) than those without symptoms.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Persistent symptoms after hospitalization are common and contribute to functional decline, falls, and ED visits in older COVID-19 survivors. These findings suggest that greater attention to symptom burden may support risk identification and improve post-discharge care planning.</p>\\n </section>\\n </div>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"73 6\",\"pages\":\"1722-1732\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2025-05-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19490\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19490\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19490","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:住院治疗经常导致老年人出现持续症状,引起人们对急性事件长期影响的担忧,这一问题因COVID-19而加剧。我们调查了持续症状对COVID-19住院康复的老年患者1年内功能下降和意外事件的影响。方法:该前瞻性队列纳入了2020年3月至12月期间在巴西最大的学术医疗中心进行的co -脆弱研究中幸存的年龄≥50岁的COVID-19住院患者。持续症状定义为入院时报告并在出院后1、3、6、9和12个月持续出现的症状,包括16种症状。结果包括基本日常生活活动(ADL)、移动活动、日常生活工具活动(IADL)、跌倒次数、急诊室(ED)就诊次数和再入院次数的功能下降。使用混合效应负二项回归模型对社会人口统计学、临床、住院相关因素和出院后康复进行调整,检验持续症状和结局之间的关系。结果:1019例患者(平均年龄65±10岁;女性= 45%;白色= 62%),324例(32%)全年持续出现症状。疲劳(28%)、肌痛(19%)和呼吸困难(13%)是最常见的症状。≥2种症状的患者活动能力功能下降的风险增加(IRR = 2.11;95% ci = 1.50-2.96), iir = 2.00;95% CI = 1.44-2.79),下降(IRR = 2.56;95% CI = 1.14-5.75),急诊科就诊(IRR = 2.69;95% CI = 1.27-5.70),但没有再入院。在女性中,≥1个持续症状与ADL下降的风险增加两倍相关。出院一年后,与没有症状的患者相比,有≥2个持续症状的患者出现了1.27个新残疾(在15点功能量表上为3.26个对1.99个),每100人年发生31个计划外事件(54.3个对23.2个)。结论:住院后持续症状很常见,并导致老年COVID-19幸存者的功能下降、跌倒和急诊就诊。这些发现表明,更多地关注症状负担可能有助于风险识别和改善出院后护理计划。
Post-Discharge COVID-19 Symptoms Predict 1-Year Functional Decline, Falls, and Emergency Department Visits: A Cohort Study
Background
Hospitalization frequently results in persistent symptoms among older adults, raising concerns about the long-term impacts of acute events—a problem amplified by COVID-19. We investigated the effects of persistent symptoms on functional decline and unplanned events over 1 year in older patients recovering from COVID-19 hospitalization.
Methods
This prospective cohort included patients aged ≥ 50 years who survived COVID-19 hospitalization between March and December 2020 as part of the CO-FRAIL study at Brazil's largest academic medical center. Persistent symptoms were defined as those reported at admission and continuously present at one-, three-, six-, nine-, and 12-month post-discharge, covering 16 symptoms. Outcomes included functional decline in basic activities of daily living (ADL), mobility activities, instrumental activities of daily living (IADL), number of falls, emergency department (ED) visits, and hospital readmissions. Associations between persistent symptoms and outcomes were examined using mixed-effects negative binomial regression models adjusted for sociodemographic, clinical, hospitalization-related factors, and post-discharge rehabilitation.
Results
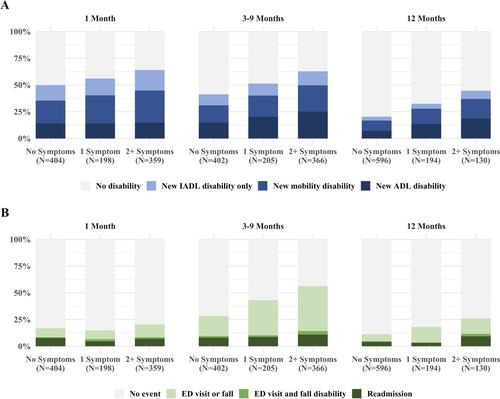
Among 1019 patients (mean age = 65 ± 10 years; women = 45%; White = 62%), 324 (32%) experienced persistent symptoms throughout the year. Fatigue (28%), myalgia (19%), and dyspnea (13%) were the most common. Patients with ≥ 2 symptoms had an increased risk of functional decline in mobility activities (IRR = 2.11; 95% CI = 1.50–2.96), IADL (IRR = 2.00; 95% CI = 1.44–2.79), falls (IRR = 2.56; 95% CI = 1.14–5.75), and ED visits (IRR = 2.69; 95% CI = 1.27–5.70), but not readmissions. Among women, ≥ 1 persistent symptom was associated with a twofold increased risk of ADL decline. One year after discharge, patients with ≥ 2 persistent symptoms developed 1.27 more new disabilities (3.26 vs. 1.99 on a 15-point functional scale) and had 31 more unplanned events per 100 person-years (54.3 vs. 23.2) than those without symptoms.
Conclusions
Persistent symptoms after hospitalization are common and contribute to functional decline, falls, and ED visits in older COVID-19 survivors. These findings suggest that greater attention to symptom burden may support risk identification and improve post-discharge care planning.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


