David C Sperling, Katrine Wallace, Nanette von Oppen, Joshua L Weintraub
{"title":"使用Y-90树脂微球治疗原发性结直肠癌不可切除肝转移患者的治疗环境从门诊医院转移到办公室实验室的预算影响","authors":"David C Sperling, Katrine Wallace, Nanette von Oppen, Joshua L Weintraub","doi":"10.2147/CEOR.S492369","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>In the wake of ever-increasing health care costs, solutions are sought to make health care more affordable, such as moving hospital outpatient procedures to office-based laboratory (OBL) settings. A budget impact model was constructed to estimate the health plan cost benefit of moving 50% of yttrium-90 resin microspheres (Y-90) selective internal radiation therapy (SIRT) procedures for unresectable liver metastases associated with primary colorectal cancer (CRC) from a traditional hospital outpatient setting (HOPPS) to an OBL setting.</p><p><strong>Methods: </strong>The eligible population was estimated using an incidence-based approach for a hypothetical health plan with 1 million covered lives. Modeled costs were based on 2024 Medicare reimbursement rates. Three treatment scenarios were considered: 1) base case HOPPS, 2) hybrid (HOPPS/OBL), and 3) OBL settings. Budget impacts were estimated as the differences in annual total cost of treatment after switching 50% of Y-90 SIRTs from HOPPS to the hybrid (HOPPS/OBL) or OBL setting. Per-member-per-month (PMPM) budget impacts were also calculated. Sensitivity analyses were conducted by varying the proportions of patients shifting settings and the treatment setting they were shifting into.</p><p><strong>Results: </strong>Annually, 28 patients were estimated to have metastatic CRC and unresectable liver metastases in a health plan of 1 million members. Average estimated per-patient cost savings would be $8,791 by switching one patient to a hybrid setting and $17,697 for a patient switched to the OBL. Switching 50% of eligible procedures resulted in PMPM cost benefits to the plan of $0.0102 for hybrid setting and $0.0206 for OBL. In sensitivity analyses, annual cost savings for the health plan were affected by both the proportion of patients shifted and the setting they were shifted into.</p><p><strong>Conclusion: </strong>Shifting a percentage of the treatment of unresectable liver metastases with Y-90 SIRT to the OBL setting results in modest cost benefits for US health plans.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"387-392"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068280/pdf/","citationCount":"0","resultStr":"{\"title\":\"Budget Impact of Shifting the Treatment Setting of Unresectable Liver Metastases Associated with Primary Colorectal Cancer Using Y-90 Resin Microspheres from the Outpatient Hospital to the Office-Based Laboratory.\",\"authors\":\"David C Sperling, Katrine Wallace, Nanette von Oppen, Joshua L Weintraub\",\"doi\":\"10.2147/CEOR.S492369\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>In the wake of ever-increasing health care costs, solutions are sought to make health care more affordable, such as moving hospital outpatient procedures to office-based laboratory (OBL) settings. A budget impact model was constructed to estimate the health plan cost benefit of moving 50% of yttrium-90 resin microspheres (Y-90) selective internal radiation therapy (SIRT) procedures for unresectable liver metastases associated with primary colorectal cancer (CRC) from a traditional hospital outpatient setting (HOPPS) to an OBL setting.</p><p><strong>Methods: </strong>The eligible population was estimated using an incidence-based approach for a hypothetical health plan with 1 million covered lives. Modeled costs were based on 2024 Medicare reimbursement rates. Three treatment scenarios were considered: 1) base case HOPPS, 2) hybrid (HOPPS/OBL), and 3) OBL settings. Budget impacts were estimated as the differences in annual total cost of treatment after switching 50% of Y-90 SIRTs from HOPPS to the hybrid (HOPPS/OBL) or OBL setting. Per-member-per-month (PMPM) budget impacts were also calculated. Sensitivity analyses were conducted by varying the proportions of patients shifting settings and the treatment setting they were shifting into.</p><p><strong>Results: </strong>Annually, 28 patients were estimated to have metastatic CRC and unresectable liver metastases in a health plan of 1 million members. Average estimated per-patient cost savings would be $8,791 by switching one patient to a hybrid setting and $17,697 for a patient switched to the OBL. Switching 50% of eligible procedures resulted in PMPM cost benefits to the plan of $0.0102 for hybrid setting and $0.0206 for OBL. In sensitivity analyses, annual cost savings for the health plan were affected by both the proportion of patients shifted and the setting they were shifted into.</p><p><strong>Conclusion: </strong>Shifting a percentage of the treatment of unresectable liver metastases with Y-90 SIRT to the OBL setting results in modest cost benefits for US health plans.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"17 \",\"pages\":\"387-392\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-05-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068280/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S492369\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S492369","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Budget Impact of Shifting the Treatment Setting of Unresectable Liver Metastases Associated with Primary Colorectal Cancer Using Y-90 Resin Microspheres from the Outpatient Hospital to the Office-Based Laboratory.
Purpose: In the wake of ever-increasing health care costs, solutions are sought to make health care more affordable, such as moving hospital outpatient procedures to office-based laboratory (OBL) settings. A budget impact model was constructed to estimate the health plan cost benefit of moving 50% of yttrium-90 resin microspheres (Y-90) selective internal radiation therapy (SIRT) procedures for unresectable liver metastases associated with primary colorectal cancer (CRC) from a traditional hospital outpatient setting (HOPPS) to an OBL setting.
Methods: The eligible population was estimated using an incidence-based approach for a hypothetical health plan with 1 million covered lives. Modeled costs were based on 2024 Medicare reimbursement rates. Three treatment scenarios were considered: 1) base case HOPPS, 2) hybrid (HOPPS/OBL), and 3) OBL settings. Budget impacts were estimated as the differences in annual total cost of treatment after switching 50% of Y-90 SIRTs from HOPPS to the hybrid (HOPPS/OBL) or OBL setting. Per-member-per-month (PMPM) budget impacts were also calculated. Sensitivity analyses were conducted by varying the proportions of patients shifting settings and the treatment setting they were shifting into.
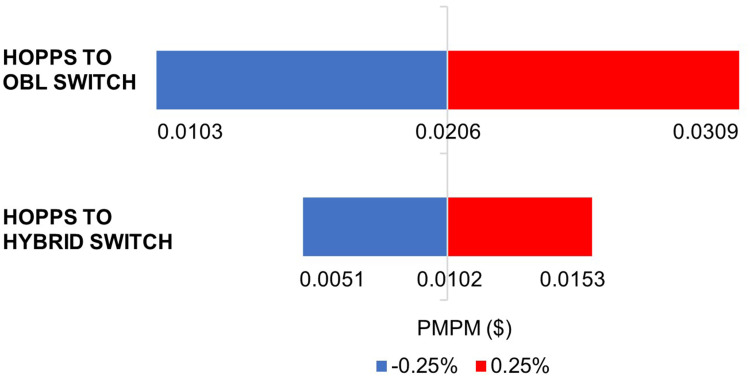
Results: Annually, 28 patients were estimated to have metastatic CRC and unresectable liver metastases in a health plan of 1 million members. Average estimated per-patient cost savings would be $8,791 by switching one patient to a hybrid setting and $17,697 for a patient switched to the OBL. Switching 50% of eligible procedures resulted in PMPM cost benefits to the plan of $0.0102 for hybrid setting and $0.0206 for OBL. In sensitivity analyses, annual cost savings for the health plan were affected by both the proportion of patients shifted and the setting they were shifted into.
Conclusion: Shifting a percentage of the treatment of unresectable liver metastases with Y-90 SIRT to the OBL setting results in modest cost benefits for US health plans.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


