Emre Kudu, Mustafa Altun, Faruk Danış, Sinan Karacabey, Erkman Sanri, Arzu Denizbasi
{"title":"验证跌倒决策规则:优化头部CT在老年人地面跌倒中的应用。","authors":"Emre Kudu, Mustafa Altun, Faruk Danış, Sinan Karacabey, Erkman Sanri, Arzu Denizbasi","doi":"10.1007/s43678-025-00937-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Falls are a leading cause of traumatic brain injury in older adults, with ground-level falls being the most common mechanism. Despite the increasing use of head computed tomography (CT) in older adults with ground-level falls, there is an ongoing debate regarding the necessity of routine neuroimaging in all cases. The falls decision rule was developed to safely exclude clinically important intracranial bleeding without head CT in older adults. This study aims to validate the falls decision rule externally and assess its accuracy in identifying low-risk patients while reducing unnecessary imaging.</p><p><strong>Methods: </strong>This prospective cohort study at a Level-1 trauma center enrolled consecutive patients aged ≥ 65 years presenting within 48 h of a ground-level fall. Patient management, including the decision to perform head CT, was determined independently by the treating emergency physician. Patients were followed up for 42 days to identify clinically important intracranial bleeding cases. The rule's diagnostic performance was evaluated using sensitivity, specificity, and predictive values using 95% confidence intervals (CI).</p><p><strong>Results: </strong>A total of 800 patients were included, with a median age of 78 years (IQR 72-85), and 59.9% were female. Clinically important intracranial bleeding was identified in 6.1% (n = 49) of patients. Head CT was performed in 67.6% of cases, identifying 43 initial hemorrhages, with six additional cases detected during follow-ups. The falls decision rule demonstrated 97.9% sensitivity (95% CI 89.1-99.9), 31.9% specificity (95% CI 28.6-35.4), and 99.5% negative predictive value (95% CI 97.1-99.9), potentially reducing CTs by one-third.</p><p><strong>Conclusion: </strong>This validation confirms the falls decision rule's high sensitivity and negative predictive value for identifying low-risk older adults after ground-level falls, potentially reducing unnecessary CT scans by approximately one-third. This approach could alleviate ED overcrowding and resource strain while ensuring diagnostic safety.</p>","PeriodicalId":93937,"journal":{"name":"CJEM","volume":" ","pages":"629-637"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380872/pdf/","citationCount":"0","resultStr":"{\"title\":\"Validating the falls decision rule: optimizing head CT use in older adults with ground-level falls.\",\"authors\":\"Emre Kudu, Mustafa Altun, Faruk Danış, Sinan Karacabey, Erkman Sanri, Arzu Denizbasi\",\"doi\":\"10.1007/s43678-025-00937-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Falls are a leading cause of traumatic brain injury in older adults, with ground-level falls being the most common mechanism. Despite the increasing use of head computed tomography (CT) in older adults with ground-level falls, there is an ongoing debate regarding the necessity of routine neuroimaging in all cases. The falls decision rule was developed to safely exclude clinically important intracranial bleeding without head CT in older adults. This study aims to validate the falls decision rule externally and assess its accuracy in identifying low-risk patients while reducing unnecessary imaging.</p><p><strong>Methods: </strong>This prospective cohort study at a Level-1 trauma center enrolled consecutive patients aged ≥ 65 years presenting within 48 h of a ground-level fall. Patient management, including the decision to perform head CT, was determined independently by the treating emergency physician. Patients were followed up for 42 days to identify clinically important intracranial bleeding cases. The rule's diagnostic performance was evaluated using sensitivity, specificity, and predictive values using 95% confidence intervals (CI).</p><p><strong>Results: </strong>A total of 800 patients were included, with a median age of 78 years (IQR 72-85), and 59.9% were female. Clinically important intracranial bleeding was identified in 6.1% (n = 49) of patients. Head CT was performed in 67.6% of cases, identifying 43 initial hemorrhages, with six additional cases detected during follow-ups. The falls decision rule demonstrated 97.9% sensitivity (95% CI 89.1-99.9), 31.9% specificity (95% CI 28.6-35.4), and 99.5% negative predictive value (95% CI 97.1-99.9), potentially reducing CTs by one-third.</p><p><strong>Conclusion: </strong>This validation confirms the falls decision rule's high sensitivity and negative predictive value for identifying low-risk older adults after ground-level falls, potentially reducing unnecessary CT scans by approximately one-third. This approach could alleviate ED overcrowding and resource strain while ensuring diagnostic safety.</p>\",\"PeriodicalId\":93937,\"journal\":{\"name\":\"CJEM\",\"volume\":\" \",\"pages\":\"629-637\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380872/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CJEM\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s43678-025-00937-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CJEM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s43678-025-00937-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/13 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:跌倒是老年人创伤性脑损伤的主要原因,地面跌倒是最常见的机制。尽管越来越多的老年人使用头部计算机断层扫描(CT)治疗地面跌倒,但对于所有病例是否需要常规神经影像学检查仍存在争议。制定跌倒判定规则是为了安全地排除老年人在没有头部CT的情况下临床上重要的颅内出血。本研究旨在外部验证跌倒决策规则,并评估其识别低风险患者的准确性,同时减少不必要的影像学检查。方法:这项在一级创伤中心进行的前瞻性队列研究纳入了年龄≥65岁的连续患者,患者在48小时内出现地面跌倒。患者的管理,包括是否进行头部CT的决定,都由负责治疗的急诊医生独立决定。随访42天,发现临床上重要的颅内出血病例。使用敏感性、特异性和95%置信区间(CI)的预测值来评估该规则的诊断性能。结果:共纳入800例患者,中位年龄78岁(IQR 72 ~ 85),女性占59.9%。临床上重要的颅内出血在6.1% (n = 49)的患者中被发现。67.6%的病例进行了头部CT检查,发现了43例初次出血,随访中发现了6例。跌倒判定规则的敏感性为97.9% (95% CI 89.1-99.9),特异性为31.9% (95% CI 28.6-35.4),阴性预测值为99.5% (95% CI 97.1-99.9),可能使ct减少三分之一。结论:该验证证实了跌倒决策规则在识别低风险老年人地面跌倒后的高敏感性和阴性预测价值,可能减少大约三分之一的不必要的CT扫描。这种方法可以缓解急诊科的拥挤和资源紧张,同时确保诊断安全。
Validating the falls decision rule: optimizing head CT use in older adults with ground-level falls.
Objective: Falls are a leading cause of traumatic brain injury in older adults, with ground-level falls being the most common mechanism. Despite the increasing use of head computed tomography (CT) in older adults with ground-level falls, there is an ongoing debate regarding the necessity of routine neuroimaging in all cases. The falls decision rule was developed to safely exclude clinically important intracranial bleeding without head CT in older adults. This study aims to validate the falls decision rule externally and assess its accuracy in identifying low-risk patients while reducing unnecessary imaging.
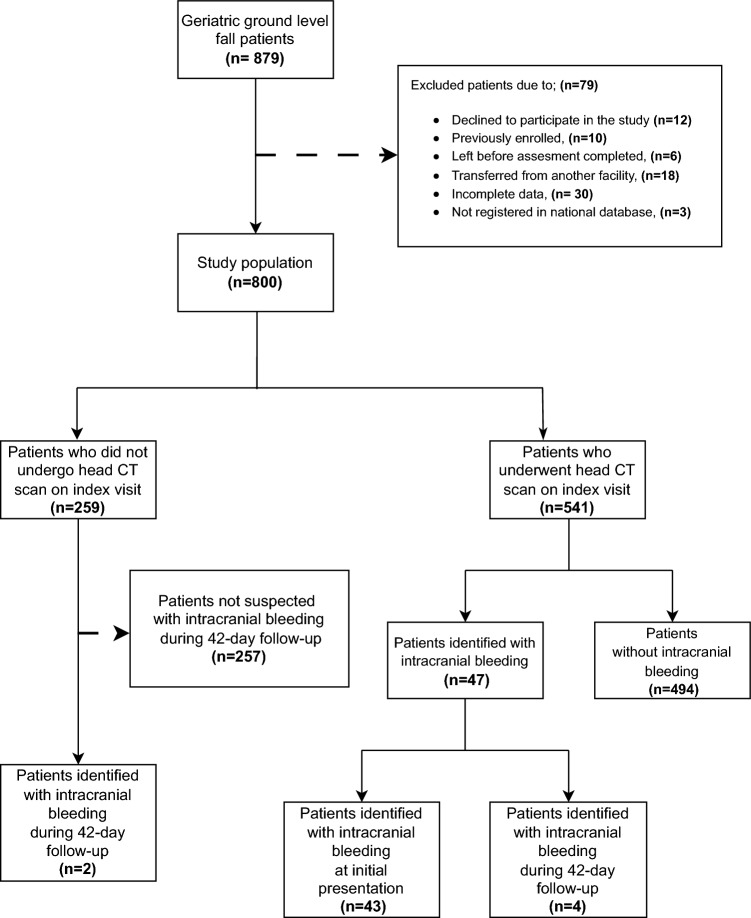
Methods: This prospective cohort study at a Level-1 trauma center enrolled consecutive patients aged ≥ 65 years presenting within 48 h of a ground-level fall. Patient management, including the decision to perform head CT, was determined independently by the treating emergency physician. Patients were followed up for 42 days to identify clinically important intracranial bleeding cases. The rule's diagnostic performance was evaluated using sensitivity, specificity, and predictive values using 95% confidence intervals (CI).
Results: A total of 800 patients were included, with a median age of 78 years (IQR 72-85), and 59.9% were female. Clinically important intracranial bleeding was identified in 6.1% (n = 49) of patients. Head CT was performed in 67.6% of cases, identifying 43 initial hemorrhages, with six additional cases detected during follow-ups. The falls decision rule demonstrated 97.9% sensitivity (95% CI 89.1-99.9), 31.9% specificity (95% CI 28.6-35.4), and 99.5% negative predictive value (95% CI 97.1-99.9), potentially reducing CTs by one-third.
Conclusion: This validation confirms the falls decision rule's high sensitivity and negative predictive value for identifying low-risk older adults after ground-level falls, potentially reducing unnecessary CT scans by approximately one-third. This approach could alleviate ED overcrowding and resource strain while ensuring diagnostic safety.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


