Vivien Chan, Adeesya Gausper, Andrew Chan-Tai-Kong, Andy M Liu, Suhas Etigunta, Justin K Scheer, Lindsay M Andras, David L Skaggs
{"title":"小儿脊柱外科侵袭性指数的建立与验证。","authors":"Vivien Chan, Adeesya Gausper, Andrew Chan-Tai-Kong, Andy M Liu, Suhas Etigunta, Justin K Scheer, Lindsay M Andras, David L Skaggs","doi":"10.1007/s43390-025-01106-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Surgical invasiveness indices have been used in adult spine surgery to characterize the invasiveness of complex procedures and for risk stratification. This has not been studied in the pediatric population. The purpose of this study was to develop and validate a surgical invasiveness index for pediatric spinal deformity surgery.</p><p><strong>Methods: </strong>The National Surgical Quality Improvement Program (NSQIP) Pediatric database was queried between the years 2016-2022. Patients were included if they were <18 years of age, received posterior or anterior-posterior spinal fusion surgery, and had a diagnosis of spinal deformity. The study cohort was divided into a derivation cohort and a validation cohort. A multivariable linear regression analysis was performed to identify surgical components associated with operative time. Surgical components of interest included number of posterior fusion levels, number of anterior fusion levels, pelvic instrumentation, posterior column osteotomies, three-column osteotomies, and prior spinal deformity surgery. Statistically significant variables were used to establish a pediatric spinal deformity surgical invasiveness index. The score was assessed and validated using linear and logistic regression analysis and receiver operating characteristic curve analysis on operative time and allogeneic transfusion.</p><p><strong>Results: </strong>There were 37,658 patients included (Derivation cohort: 26,372; Validation cohort: 11,286). In the linear regression analysis, more posterior fusion levels (7-12 levels: 0.54, p<0.001;>12 levels: 1.40, p<0.001), anterior fusion 1-3 levels (2.42, p<0.001), anterior fusion ≥4 levels (2.93, p<0.001), pelvic instrumentation (0.79, p<0.001), and previous spinal deformity surgery (0.44, p<0.001) were associated with longer operative time. Each level of posterior column osteotomy (0.13, p<0.001) and three-column osteotomy (0.61, p<0.001) were associated with increased operative time. Points were assigned to each surgical component: 7-12 posterior fusion levels (4 pts), >12 posterior fusion levels (11 pts), anterior fusion 1-3 levels (19 pts), anterior fusion ≥4 levels (23 pts), pelvic instrumentation (6 pts), previous spinal deformity surgery (3 pts), posterior column osteotomy (1 pt per level), and three-column osteotomy (5 pts per level). In the derivation cohort, each point was associated with an increase in operative time by 0.13 hours (R<sup>2</sup>=0.16, p<0.001). In the validation cohort, each point was associated with an increase in operative time by 0.12 hours (R<sup>2</sup>=0.15, p<0.001). In the derivation cohort, the area under the curve (AUC) for operative time ≥8 hours and allogeneic transfusion were 0.74 and 0.71, respectively. In the validation cohort, the AUC for operative time ≥8 hours and allogeneic transfusion were 0.74 and 0.70, respectively.</p><p><strong>Conclusion: </strong>A pediatric spinal deformity surgical invasiveness index was created and predictive of prolonged operative time and allogeneic transfusion. This is the first quantitative tool to measure the extent of surgical interventions in pediatric spine surgery.</p>","PeriodicalId":21796,"journal":{"name":"Spine deformity","volume":" ","pages":"1367-1376"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401766/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and validation of a pediatric spine surgical invasiveness index.\",\"authors\":\"Vivien Chan, Adeesya Gausper, Andrew Chan-Tai-Kong, Andy M Liu, Suhas Etigunta, Justin K Scheer, Lindsay M Andras, David L Skaggs\",\"doi\":\"10.1007/s43390-025-01106-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Surgical invasiveness indices have been used in adult spine surgery to characterize the invasiveness of complex procedures and for risk stratification. This has not been studied in the pediatric population. The purpose of this study was to develop and validate a surgical invasiveness index for pediatric spinal deformity surgery.</p><p><strong>Methods: </strong>The National Surgical Quality Improvement Program (NSQIP) Pediatric database was queried between the years 2016-2022. Patients were included if they were <18 years of age, received posterior or anterior-posterior spinal fusion surgery, and had a diagnosis of spinal deformity. The study cohort was divided into a derivation cohort and a validation cohort. A multivariable linear regression analysis was performed to identify surgical components associated with operative time. Surgical components of interest included number of posterior fusion levels, number of anterior fusion levels, pelvic instrumentation, posterior column osteotomies, three-column osteotomies, and prior spinal deformity surgery. Statistically significant variables were used to establish a pediatric spinal deformity surgical invasiveness index. The score was assessed and validated using linear and logistic regression analysis and receiver operating characteristic curve analysis on operative time and allogeneic transfusion.</p><p><strong>Results: </strong>There were 37,658 patients included (Derivation cohort: 26,372; Validation cohort: 11,286). In the linear regression analysis, more posterior fusion levels (7-12 levels: 0.54, p<0.001;>12 levels: 1.40, p<0.001), anterior fusion 1-3 levels (2.42, p<0.001), anterior fusion ≥4 levels (2.93, p<0.001), pelvic instrumentation (0.79, p<0.001), and previous spinal deformity surgery (0.44, p<0.001) were associated with longer operative time. Each level of posterior column osteotomy (0.13, p<0.001) and three-column osteotomy (0.61, p<0.001) were associated with increased operative time. Points were assigned to each surgical component: 7-12 posterior fusion levels (4 pts), >12 posterior fusion levels (11 pts), anterior fusion 1-3 levels (19 pts), anterior fusion ≥4 levels (23 pts), pelvic instrumentation (6 pts), previous spinal deformity surgery (3 pts), posterior column osteotomy (1 pt per level), and three-column osteotomy (5 pts per level). In the derivation cohort, each point was associated with an increase in operative time by 0.13 hours (R<sup>2</sup>=0.16, p<0.001). In the validation cohort, each point was associated with an increase in operative time by 0.12 hours (R<sup>2</sup>=0.15, p<0.001). In the derivation cohort, the area under the curve (AUC) for operative time ≥8 hours and allogeneic transfusion were 0.74 and 0.71, respectively. In the validation cohort, the AUC for operative time ≥8 hours and allogeneic transfusion were 0.74 and 0.70, respectively.</p><p><strong>Conclusion: </strong>A pediatric spinal deformity surgical invasiveness index was created and predictive of prolonged operative time and allogeneic transfusion. This is the first quantitative tool to measure the extent of surgical interventions in pediatric spine surgery.</p>\",\"PeriodicalId\":21796,\"journal\":{\"name\":\"Spine deformity\",\"volume\":\" \",\"pages\":\"1367-1376\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401766/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine deformity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s43390-025-01106-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine deformity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s43390-025-01106-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/13 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Development and validation of a pediatric spine surgical invasiveness index.
Purpose: Surgical invasiveness indices have been used in adult spine surgery to characterize the invasiveness of complex procedures and for risk stratification. This has not been studied in the pediatric population. The purpose of this study was to develop and validate a surgical invasiveness index for pediatric spinal deformity surgery.
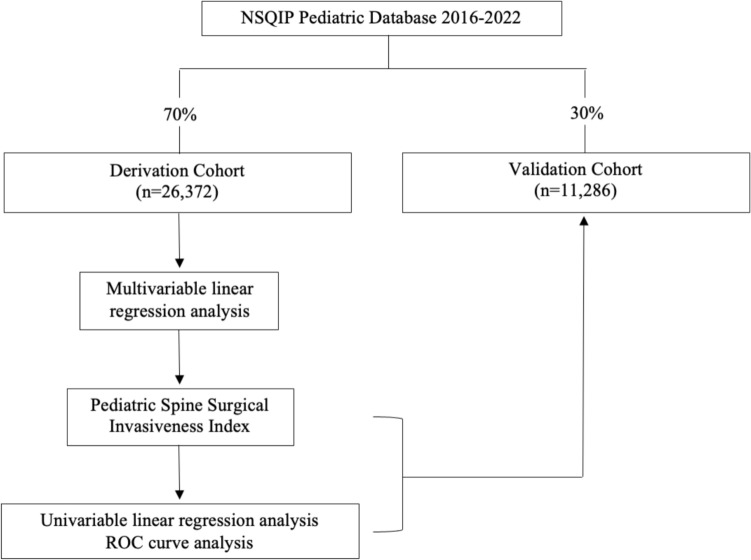
Methods: The National Surgical Quality Improvement Program (NSQIP) Pediatric database was queried between the years 2016-2022. Patients were included if they were <18 years of age, received posterior or anterior-posterior spinal fusion surgery, and had a diagnosis of spinal deformity. The study cohort was divided into a derivation cohort and a validation cohort. A multivariable linear regression analysis was performed to identify surgical components associated with operative time. Surgical components of interest included number of posterior fusion levels, number of anterior fusion levels, pelvic instrumentation, posterior column osteotomies, three-column osteotomies, and prior spinal deformity surgery. Statistically significant variables were used to establish a pediatric spinal deformity surgical invasiveness index. The score was assessed and validated using linear and logistic regression analysis and receiver operating characteristic curve analysis on operative time and allogeneic transfusion.
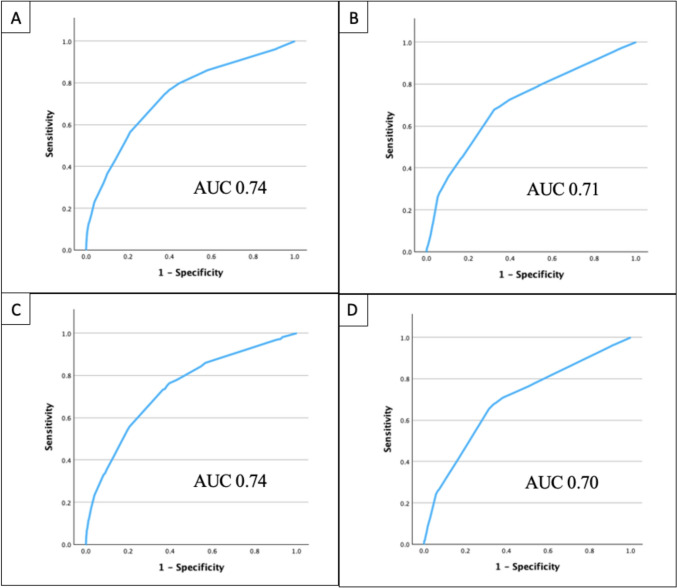
Results: There were 37,658 patients included (Derivation cohort: 26,372; Validation cohort: 11,286). In the linear regression analysis, more posterior fusion levels (7-12 levels: 0.54, p<0.001;>12 levels: 1.40, p<0.001), anterior fusion 1-3 levels (2.42, p<0.001), anterior fusion ≥4 levels (2.93, p<0.001), pelvic instrumentation (0.79, p<0.001), and previous spinal deformity surgery (0.44, p<0.001) were associated with longer operative time. Each level of posterior column osteotomy (0.13, p<0.001) and three-column osteotomy (0.61, p<0.001) were associated with increased operative time. Points were assigned to each surgical component: 7-12 posterior fusion levels (4 pts), >12 posterior fusion levels (11 pts), anterior fusion 1-3 levels (19 pts), anterior fusion ≥4 levels (23 pts), pelvic instrumentation (6 pts), previous spinal deformity surgery (3 pts), posterior column osteotomy (1 pt per level), and three-column osteotomy (5 pts per level). In the derivation cohort, each point was associated with an increase in operative time by 0.13 hours (R2=0.16, p<0.001). In the validation cohort, each point was associated with an increase in operative time by 0.12 hours (R2=0.15, p<0.001). In the derivation cohort, the area under the curve (AUC) for operative time ≥8 hours and allogeneic transfusion were 0.74 and 0.71, respectively. In the validation cohort, the AUC for operative time ≥8 hours and allogeneic transfusion were 0.74 and 0.70, respectively.
Conclusion: A pediatric spinal deformity surgical invasiveness index was created and predictive of prolonged operative time and allogeneic transfusion. This is the first quantitative tool to measure the extent of surgical interventions in pediatric spine surgery.
期刊介绍:
Spine Deformity the official journal of the?Scoliosis Research Society is a peer-refereed publication to disseminate knowledge on basic science and clinical research into the?etiology?biomechanics?treatment?methods and outcomes of all types of?spinal deformities. The international members of the Editorial Board provide a worldwide perspective for the journal's area of interest.The?journal?will enhance the mission of the Society which is to foster the optimal care of all patients with?spine?deformities worldwide. Articles published in?Spine Deformity?are Medline indexed in PubMed.? The journal publishes original articles in the form of clinical and basic research. Spine Deformity will only publish studies that have institutional review board (IRB) or similar ethics committee approval for human and animal studies and have strictly observed these guidelines. The minimum follow-up period for follow-up clinical studies is 24 months.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


