Mars Yixing Zhao, Samuel Girgis, Thomas Goldade, Evan Parchomchuk, Michaela Nickol, Johannes M van der Merwe
{"title":"血清学和滑膜试验对假体周围关节感染的比较诊断价值:综合分析。","authors":"Mars Yixing Zhao, Samuel Girgis, Thomas Goldade, Evan Parchomchuk, Michaela Nickol, Johannes M van der Merwe","doi":"10.2106/JBJS.OA.24.00206","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prompt diagnosis of periprosthetic joint infections (PJIs) is crucial for providing optimal care. Currently, there are no gold-standard tests available. An ideal test would be simple to implement, cost-effective, and readily available. We aimed to determine the best single or combined serological or synovial markers for diagnosing PJIs.</p><p><strong>Methods: </strong>There were 177 of 313 patients who had PJIs between April 2012 and March 2023 and a control group of 60 patients who were included in this retrospective review. The PJIs were diagnosed using Musculoskeletal Infection Society (MSIS) and European Bone and Joint Infection Society (EBJIS) criteria. Serum (C-reactive protein [CRP], white blood-cell [WBC] count, neutrophil-lymphocyte ratio [NLR], polymorphonuclear neutrophil percentage [PMN%]), and synovial fluid (WBC, NLR, PMN%) parameters were compared between the 2 groups. We determined the sensitivity, specificity, area under the curve (AUC), and cutoff values (COV) for each marker. We determined the best combination of markers to diagnose PJIs. There was no statistical significance between the demographic data of the control and treatment groups.</p><p><strong>Results: </strong>The S-CRP had the highest AUC of 0.912 with a COV of 16.15 mg/dL (Sensitivity 79.6%, Specificity 97.8%). The combination of tests, S-CRP, synovial fluid (SF-WBC), and S-NLR demonstrated the highest AUC of 0.946 (Sensitivity 93%, Specificity 90.9%). The COV for SF-WBC was 5.75 cells/μL (AUC 0.803; Sensitivity 70.3%, Specificity 97.1%); S-NLR COV was 3.659 (AUC 0.803; Sensitivity 67.3%, Specificity 88%).</p><p><strong>Conclusion: </strong>We found the combination of S-CRP, SF-WBC, and S-NLR to be valuable in diagnosing PJI with high sensitivities and specificities. It can be easily implemented by clinicians without additional cost or equipment. It is important to use this with a thorough clinical and physical examination as well as other modalities (i.e., MSIS/EBJIS criteria).</p><p><strong>Level of evidence: </strong>Retrospective Comparative Study-Level III evidence. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 2","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020709/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative Diagnostic Value of Serological and Synovial Tests for Periprosthetic Joint Infections: A Comprehensive Analysis.\",\"authors\":\"Mars Yixing Zhao, Samuel Girgis, Thomas Goldade, Evan Parchomchuk, Michaela Nickol, Johannes M van der Merwe\",\"doi\":\"10.2106/JBJS.OA.24.00206\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prompt diagnosis of periprosthetic joint infections (PJIs) is crucial for providing optimal care. Currently, there are no gold-standard tests available. An ideal test would be simple to implement, cost-effective, and readily available. We aimed to determine the best single or combined serological or synovial markers for diagnosing PJIs.</p><p><strong>Methods: </strong>There were 177 of 313 patients who had PJIs between April 2012 and March 2023 and a control group of 60 patients who were included in this retrospective review. The PJIs were diagnosed using Musculoskeletal Infection Society (MSIS) and European Bone and Joint Infection Society (EBJIS) criteria. Serum (C-reactive protein [CRP], white blood-cell [WBC] count, neutrophil-lymphocyte ratio [NLR], polymorphonuclear neutrophil percentage [PMN%]), and synovial fluid (WBC, NLR, PMN%) parameters were compared between the 2 groups. We determined the sensitivity, specificity, area under the curve (AUC), and cutoff values (COV) for each marker. We determined the best combination of markers to diagnose PJIs. There was no statistical significance between the demographic data of the control and treatment groups.</p><p><strong>Results: </strong>The S-CRP had the highest AUC of 0.912 with a COV of 16.15 mg/dL (Sensitivity 79.6%, Specificity 97.8%). The combination of tests, S-CRP, synovial fluid (SF-WBC), and S-NLR demonstrated the highest AUC of 0.946 (Sensitivity 93%, Specificity 90.9%). The COV for SF-WBC was 5.75 cells/μL (AUC 0.803; Sensitivity 70.3%, Specificity 97.1%); S-NLR COV was 3.659 (AUC 0.803; Sensitivity 67.3%, Specificity 88%).</p><p><strong>Conclusion: </strong>We found the combination of S-CRP, SF-WBC, and S-NLR to be valuable in diagnosing PJI with high sensitivities and specificities. It can be easily implemented by clinicians without additional cost or equipment. It is important to use this with a thorough clinical and physical examination as well as other modalities (i.e., MSIS/EBJIS criteria).</p><p><strong>Level of evidence: </strong>Retrospective Comparative Study-Level III evidence. See Instructions for Authors for a complete description of levels of evidence.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"10 2\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020709/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.24.00206\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.24.00206","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Comparative Diagnostic Value of Serological and Synovial Tests for Periprosthetic Joint Infections: A Comprehensive Analysis.
Background: Prompt diagnosis of periprosthetic joint infections (PJIs) is crucial for providing optimal care. Currently, there are no gold-standard tests available. An ideal test would be simple to implement, cost-effective, and readily available. We aimed to determine the best single or combined serological or synovial markers for diagnosing PJIs.
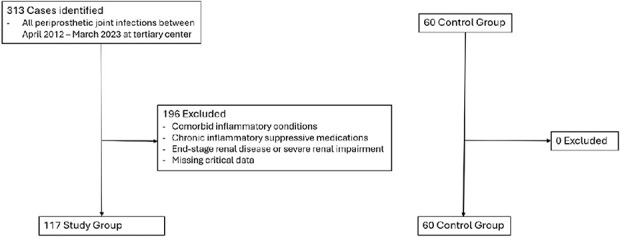
Methods: There were 177 of 313 patients who had PJIs between April 2012 and March 2023 and a control group of 60 patients who were included in this retrospective review. The PJIs were diagnosed using Musculoskeletal Infection Society (MSIS) and European Bone and Joint Infection Society (EBJIS) criteria. Serum (C-reactive protein [CRP], white blood-cell [WBC] count, neutrophil-lymphocyte ratio [NLR], polymorphonuclear neutrophil percentage [PMN%]), and synovial fluid (WBC, NLR, PMN%) parameters were compared between the 2 groups. We determined the sensitivity, specificity, area under the curve (AUC), and cutoff values (COV) for each marker. We determined the best combination of markers to diagnose PJIs. There was no statistical significance between the demographic data of the control and treatment groups.
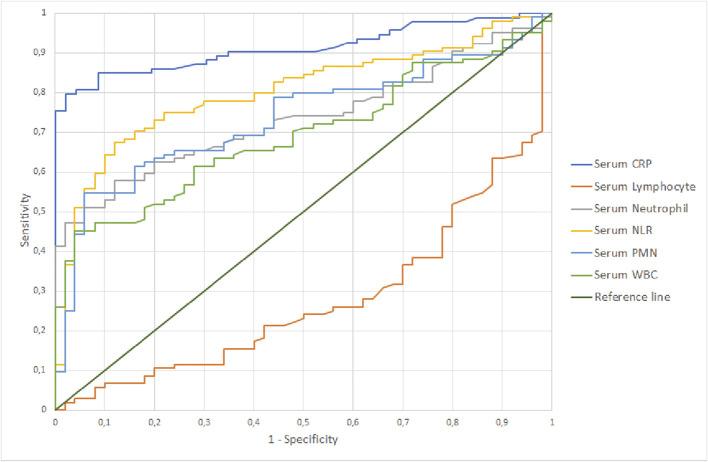
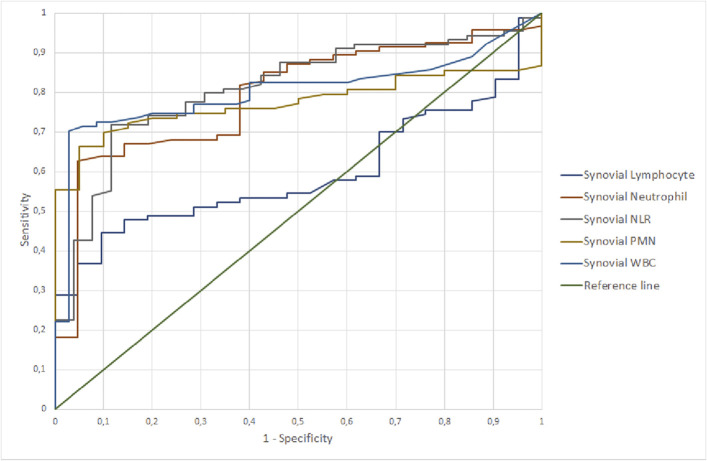
Results: The S-CRP had the highest AUC of 0.912 with a COV of 16.15 mg/dL (Sensitivity 79.6%, Specificity 97.8%). The combination of tests, S-CRP, synovial fluid (SF-WBC), and S-NLR demonstrated the highest AUC of 0.946 (Sensitivity 93%, Specificity 90.9%). The COV for SF-WBC was 5.75 cells/μL (AUC 0.803; Sensitivity 70.3%, Specificity 97.1%); S-NLR COV was 3.659 (AUC 0.803; Sensitivity 67.3%, Specificity 88%).
Conclusion: We found the combination of S-CRP, SF-WBC, and S-NLR to be valuable in diagnosing PJI with high sensitivities and specificities. It can be easily implemented by clinicians without additional cost or equipment. It is important to use this with a thorough clinical and physical examination as well as other modalities (i.e., MSIS/EBJIS criteria).
Level of evidence: Retrospective Comparative Study-Level III evidence. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


