Victor M Wauye, G Titus Ngeno, Chrispine O Oduor, Felix A Barasa
{"title":"肯尼亚一家公立三级医院急性失代偿性心力衰竭入院的成人心力衰竭的主要原因和直接医疗费用","authors":"Victor M Wauye, G Titus Ngeno, Chrispine O Oduor, Felix A Barasa","doi":"10.5334/gh.1426","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Heart failure (HF) is a major contributor to cardiovascular morbidity and mortality. Adversely impacting health outcomes in Kenya and other developing countries, data on the direct medical cost of HF hospitalization remain limited.</p><p><strong>Methods: </strong>This was a prospective study conducted at Moi Teaching and Referral Hospital. Patients with HF were identified by sequential medical chart abstraction. Primary causes were extracted from echocardiogram reports and adjudicated by a cardiologist. Direct medical cost of hospitalization was derived using activity-based and micro-costing methods, adopting payers' system perspective. Drivers of overall cost were explored using linear regression models.</p><p><strong>Results: </strong>142 participants were consecutively recruited from September to November 2022. 51.4% were females, and the mean age was 54 (SD 20). The leading primary causes were cor pulmonale (CP), 28.9%; dilated cardiomyopathy (DCM), 26.1%; rheumatic heart disease (RHD), 19.7%; hypertensive heart disease (HHD), 16.9%; ischaemic heart disease (IHD), 6.3%; and pericardial disease (PD), 2.1%. Overall direct cost of HF hospitalization was KES 11,470.94 (SD 8,289.57) [USD 93.49 (67.56)] per patient per day, with the mean length of hospital stay of 10.1 (SD 7.1). RHD incurred the highest costs, KES 15,299.08 (SD 13,196.89) [USD 124.70 (107.56)] per patient per day; IHD, KES 12,966.47 (SD 6656.49) [USD 105.68 (54.25)]; and DCM, KES 12,268.08 (SD 7,816.12) [USD 99.99 (63.71)]. The cost of medications was the leading driver, β = 0.56 (0.55 - 0.56), followed by inpatient fees, β = 0.27 (0.27 - 0.28), and laboratory investigations, β = 0.19 (0.18 - 0.19).</p><p><strong>Conclusion: </strong>Cor pulmonale, CM, RHD, and HHD were the major causes of HF. The overall direct medical cost of hospitalization was extremely expensive compared with the Kenyan average monthly household income per capita. Widespread comprehensive health insurance coverage is therefore recommended to cushion families against such catastrophic health expenditures besides public health measures aimed at addressing primary causes of HF.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"42"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12047636/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary Causes and Direct Medical Cost of Heart Failure Among Adults Admitted with Acute Decompensated Heart Failure in a Public Tertiary Hospital, Kenya.\",\"authors\":\"Victor M Wauye, G Titus Ngeno, Chrispine O Oduor, Felix A Barasa\",\"doi\":\"10.5334/gh.1426\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Heart failure (HF) is a major contributor to cardiovascular morbidity and mortality. Adversely impacting health outcomes in Kenya and other developing countries, data on the direct medical cost of HF hospitalization remain limited.</p><p><strong>Methods: </strong>This was a prospective study conducted at Moi Teaching and Referral Hospital. Patients with HF were identified by sequential medical chart abstraction. Primary causes were extracted from echocardiogram reports and adjudicated by a cardiologist. Direct medical cost of hospitalization was derived using activity-based and micro-costing methods, adopting payers' system perspective. Drivers of overall cost were explored using linear regression models.</p><p><strong>Results: </strong>142 participants were consecutively recruited from September to November 2022. 51.4% were females, and the mean age was 54 (SD 20). The leading primary causes were cor pulmonale (CP), 28.9%; dilated cardiomyopathy (DCM), 26.1%; rheumatic heart disease (RHD), 19.7%; hypertensive heart disease (HHD), 16.9%; ischaemic heart disease (IHD), 6.3%; and pericardial disease (PD), 2.1%. Overall direct cost of HF hospitalization was KES 11,470.94 (SD 8,289.57) [USD 93.49 (67.56)] per patient per day, with the mean length of hospital stay of 10.1 (SD 7.1). RHD incurred the highest costs, KES 15,299.08 (SD 13,196.89) [USD 124.70 (107.56)] per patient per day; IHD, KES 12,966.47 (SD 6656.49) [USD 105.68 (54.25)]; and DCM, KES 12,268.08 (SD 7,816.12) [USD 99.99 (63.71)]. The cost of medications was the leading driver, β = 0.56 (0.55 - 0.56), followed by inpatient fees, β = 0.27 (0.27 - 0.28), and laboratory investigations, β = 0.19 (0.18 - 0.19).</p><p><strong>Conclusion: </strong>Cor pulmonale, CM, RHD, and HHD were the major causes of HF. The overall direct medical cost of hospitalization was extremely expensive compared with the Kenyan average monthly household income per capita. Widespread comprehensive health insurance coverage is therefore recommended to cushion families against such catastrophic health expenditures besides public health measures aimed at addressing primary causes of HF.</p>\",\"PeriodicalId\":56018,\"journal\":{\"name\":\"Global Heart\",\"volume\":\"20 1\",\"pages\":\"42\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12047636/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Heart\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5334/gh.1426\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1426","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Primary Causes and Direct Medical Cost of Heart Failure Among Adults Admitted with Acute Decompensated Heart Failure in a Public Tertiary Hospital, Kenya.
Background: Heart failure (HF) is a major contributor to cardiovascular morbidity and mortality. Adversely impacting health outcomes in Kenya and other developing countries, data on the direct medical cost of HF hospitalization remain limited.
Methods: This was a prospective study conducted at Moi Teaching and Referral Hospital. Patients with HF were identified by sequential medical chart abstraction. Primary causes were extracted from echocardiogram reports and adjudicated by a cardiologist. Direct medical cost of hospitalization was derived using activity-based and micro-costing methods, adopting payers' system perspective. Drivers of overall cost were explored using linear regression models.
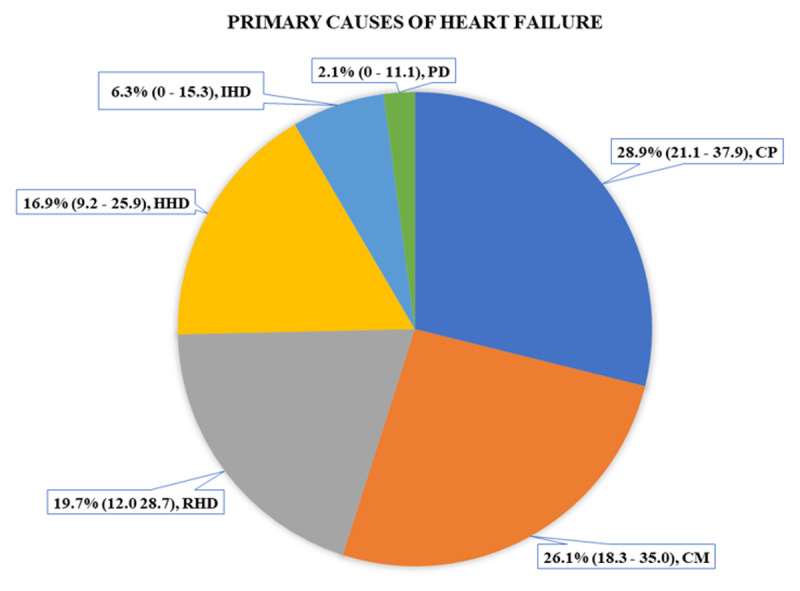
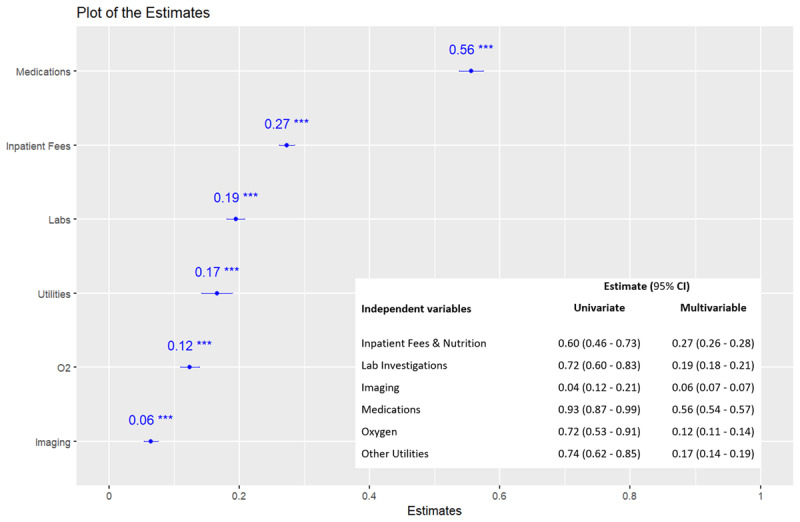
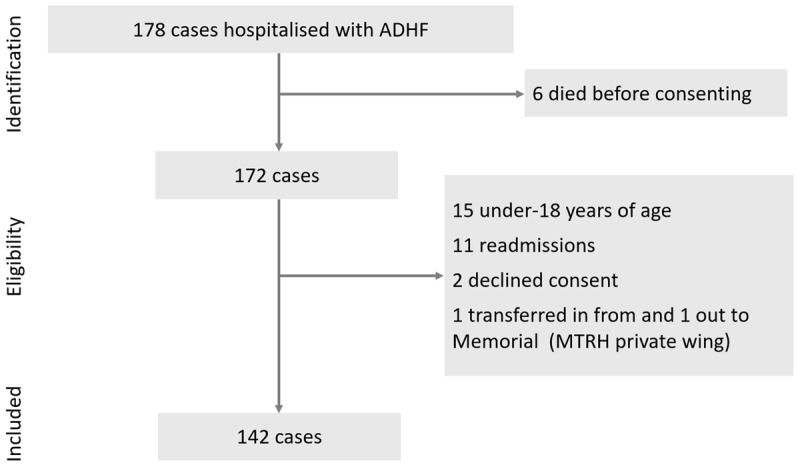
Results: 142 participants were consecutively recruited from September to November 2022. 51.4% were females, and the mean age was 54 (SD 20). The leading primary causes were cor pulmonale (CP), 28.9%; dilated cardiomyopathy (DCM), 26.1%; rheumatic heart disease (RHD), 19.7%; hypertensive heart disease (HHD), 16.9%; ischaemic heart disease (IHD), 6.3%; and pericardial disease (PD), 2.1%. Overall direct cost of HF hospitalization was KES 11,470.94 (SD 8,289.57) [USD 93.49 (67.56)] per patient per day, with the mean length of hospital stay of 10.1 (SD 7.1). RHD incurred the highest costs, KES 15,299.08 (SD 13,196.89) [USD 124.70 (107.56)] per patient per day; IHD, KES 12,966.47 (SD 6656.49) [USD 105.68 (54.25)]; and DCM, KES 12,268.08 (SD 7,816.12) [USD 99.99 (63.71)]. The cost of medications was the leading driver, β = 0.56 (0.55 - 0.56), followed by inpatient fees, β = 0.27 (0.27 - 0.28), and laboratory investigations, β = 0.19 (0.18 - 0.19).
Conclusion: Cor pulmonale, CM, RHD, and HHD were the major causes of HF. The overall direct medical cost of hospitalization was extremely expensive compared with the Kenyan average monthly household income per capita. Widespread comprehensive health insurance coverage is therefore recommended to cushion families against such catastrophic health expenditures besides public health measures aimed at addressing primary causes of HF.
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


