Prediction of small-for-gestational age and fetal growth restriction at routine ultrasound examination at 35-37 weeks' gestation.
Objective: To evaluate the performance of sonographic fetal biometry and Doppler parameters assessed at routine third-trimester ultrasound examination for predicting small-for-gestational age (SGA) and fetal growth restriction (FGR).
Methods: This was a retrospective cohort study of low-risk singleton pregnancies undergoing routine ultrasound examination between 35 + 0 and 37 + 6 weeks' gestation and delivered at St George's University Hospital, London, UK, between December 2019 and February 2024. The study outcomes were SGA (birth weight < 5th centile) and FGR (birth weight < 3rd centile or birth weight < 10th centile with composite adverse perinatal outcome). Composite adverse perinatal outcome comprised intrauterine death, neonatal death or admission to the neonatal intensive care unit. Demographic characteristics, estimated fetal weight (EFW) and abdominal circumference centiles, as well as Doppler indices, including pulsatility indices (PI) of the umbilical artery (UA), middle cerebral artery (MCA) and uterine artery (UtA) were evaluated. The cerebroplacental ratio (CPR) was calculated, and all indices were converted to multiples of the median (MoM). Multivariable logistic regression analysis was performed to identify and adjust for confounders. The area under the receiver-operating-characteristics curve (AUC) was used to evaluate the model's performance for predicting small neonates.
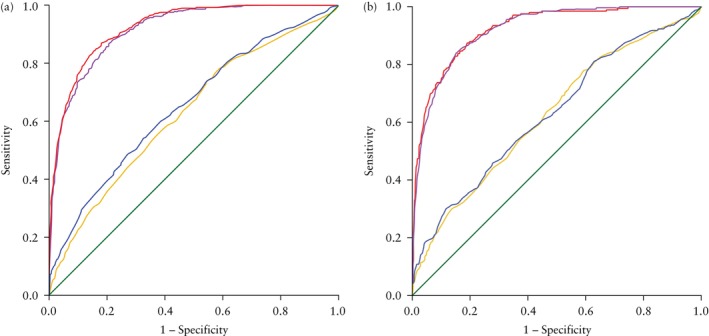
Results: A total of 14 161 pregnancies were included in the study. The prevalence of SGA and FGR neonates was 3.1% and 1.5%, respectively. Independent predictors of SGA and FGR, respectively, were: EFW centile (adjusted odds ratio (aOR) 0.91 (95% CI, 0.90-0.92); P < 0.001 and aOR 0.90 (95% CI, 0.89-0.91); P < 0.001); AC centile (aOR 0.91 (95% CI, 0.90-0.92); P < 0.001 and aOR 0.91 (95% CI, 0.90-0.92); P <0.001); UA-PI MoM (aOR 4.60 (95% CI, 2.19-9.64); P < 0.001 and aOR 2.53 (95% CI, 1.05-6.10); P = 0.038); MCA-PI MoM (aOR 0.37 (95% CI, 0.20-0.70); P = 0.002 and aOR 0.26 (95% CI, 0.12-0.59); P = 0.001); CPR MoM (aOR 0.23 (95% CI, 0.13-0.42); P < 0.001 and aOR 0.25 (95% CI, 0.12-0.53); P < 0.001); and UtA-PI MoM (aOR 2.54 (95% CI, 1.68-3.83); P < 0.001 and aOR 2.16 (95% CI, 1.31-3.58); P = 0.003). The EFW centile alone was associated with an AUC of 0.917 (95% CI, 0.907-0.929) for the prediction of SGA and 0.925 (95% CI, 0.908-0.939) for the prediction of FGR. This was similar to AUCs of around 0.92 for the prediction of SGA and AUCs of around 0.93 for the prediction of FGR when the EFW centile was combined with any Doppler parameters.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


