{"title":"腹会阴直肠癌切除术后肿瘤位置对预后的影响:基于1806例病例的单中心倾向评分匹配分析","authors":"Zixing Zhu, Chunbing Wang, Dedi Jiang, Zhixun Zhao, Jianjun Bi, Qiang Feng, Wei Pei, Haitao Zhou, Zhaoxu Zheng, Qian Liu, Jichuan Quan, Jianwei Liang","doi":"10.1007/s10151-025-03114-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Randomized controlled trials have revealed that abdominoperineal resection leads to inferior oncological outcomes compared with low anterior resection, especially regarding local recurrence rates (LRRs). While neoadjuvant chemoradiotherapy can lower LRRs, it is linked to potential short- and long-term radiation-induced adverse effects. Consequently, meticulous patient selection for neoadjuvant chemoradiotherapy is imperative to balance benefits and risks.</p><p><strong>Methods: </strong>This research encompassed individuals with rectal cancer (RC) who underwent abdominoperineal resection (APR) from January 2006 to December 2017. The cohort was categorized into two cohorts on the basis of tumor location: the anterior cohort and the nonanterior cohort. Propensity score matching (PSM) was employed to mitigate selection bias, and this resulted in 767 patients in both cohorts. The primary endpoint assessed was survival without local recurrence (LR).</p><p><strong>Results: </strong>Of the 2025 cases examined, 1806 were deemed eligible for inclusion. In the entire cohort, the incidence of LR was 9.9% (178/1806); the anterior cohort exhibited a higher rate of LR (15.2% versus 5.9%, p < 0.001). Multivariate examination revealed that anterior location was an independent risk factor (IRF) for LR (hazard ratio [HR] = 2.503, p < 0.001). In patients with stage II/III or T3/4, anterior location persisted as a predictor of increased LR. Neoadjuvant chemoradiotherapy for stage II and III tumors diminished the LR rate in anterior tumor locations (p = 0.017) but not in nonanterior locations (p = 0.390).</p><p><strong>Conclusion: </strong>Anterior tumor location is an IRF for LR in RC patients. Tumor location can serve as a criterion for patient selection in neoadjuvant chemoradiotherapy.</p><p><strong>Trial registration: </strong>The studies involving human participants were reviewed and approved by the National Cancer Center's Institute Research Medical Ethics Committee (23/180-3922, 11 May 2023). A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.</p>","PeriodicalId":51192,"journal":{"name":"Techniques in Coloproctology","volume":"29 1","pages":"99"},"PeriodicalIF":2.9000,"publicationDate":"2025-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982106/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic impact of tumor location after abdominoperineal resection of rectal cancer: A single-center propensity score matching analysis based on 1806 cases.\",\"authors\":\"Zixing Zhu, Chunbing Wang, Dedi Jiang, Zhixun Zhao, Jianjun Bi, Qiang Feng, Wei Pei, Haitao Zhou, Zhaoxu Zheng, Qian Liu, Jichuan Quan, Jianwei Liang\",\"doi\":\"10.1007/s10151-025-03114-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Randomized controlled trials have revealed that abdominoperineal resection leads to inferior oncological outcomes compared with low anterior resection, especially regarding local recurrence rates (LRRs). While neoadjuvant chemoradiotherapy can lower LRRs, it is linked to potential short- and long-term radiation-induced adverse effects. Consequently, meticulous patient selection for neoadjuvant chemoradiotherapy is imperative to balance benefits and risks.</p><p><strong>Methods: </strong>This research encompassed individuals with rectal cancer (RC) who underwent abdominoperineal resection (APR) from January 2006 to December 2017. The cohort was categorized into two cohorts on the basis of tumor location: the anterior cohort and the nonanterior cohort. Propensity score matching (PSM) was employed to mitigate selection bias, and this resulted in 767 patients in both cohorts. The primary endpoint assessed was survival without local recurrence (LR).</p><p><strong>Results: </strong>Of the 2025 cases examined, 1806 were deemed eligible for inclusion. In the entire cohort, the incidence of LR was 9.9% (178/1806); the anterior cohort exhibited a higher rate of LR (15.2% versus 5.9%, p < 0.001). Multivariate examination revealed that anterior location was an independent risk factor (IRF) for LR (hazard ratio [HR] = 2.503, p < 0.001). In patients with stage II/III or T3/4, anterior location persisted as a predictor of increased LR. Neoadjuvant chemoradiotherapy for stage II and III tumors diminished the LR rate in anterior tumor locations (p = 0.017) but not in nonanterior locations (p = 0.390).</p><p><strong>Conclusion: </strong>Anterior tumor location is an IRF for LR in RC patients. Tumor location can serve as a criterion for patient selection in neoadjuvant chemoradiotherapy.</p><p><strong>Trial registration: </strong>The studies involving human participants were reviewed and approved by the National Cancer Center's Institute Research Medical Ethics Committee (23/180-3922, 11 May 2023). A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.</p>\",\"PeriodicalId\":51192,\"journal\":{\"name\":\"Techniques in Coloproctology\",\"volume\":\"29 1\",\"pages\":\"99\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-04-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982106/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Techniques in Coloproctology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10151-025-03114-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Techniques in Coloproctology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10151-025-03114-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:随机对照试验显示,与低前切除术相比,腹会阴切除术的肿瘤预后较差,特别是在局部复发率(lrr)方面。虽然新辅助放化疗可以降低lrr,但它与潜在的短期和长期辐射引起的不良反应有关。因此,细致的患者选择新辅助放化疗是必要的,以平衡利益和风险。方法:本研究纳入了2006年1月至2017年12月接受腹部会阴切除术(APR)的直肠癌(RC)患者。根据肿瘤位置将队列分为前路队列和非前路队列。采用倾向评分匹配(PSM)来减轻选择偏倚,这导致两个队列中有767例患者。评估的主要终点是无局部复发的生存期(LR)。结果:在研究的2025例病例中,1806例被认为符合纳入条件。在整个队列中,LR的发生率为9.9% (178/1806);前路组的LR发生率更高(15.2% vs 5.9%)。结论:肿瘤前位是RC患者LR的IRF。肿瘤位置可作为新辅助放化疗患者选择的标准。试验注册:涉及人类受试者的研究由国家癌症中心研究所医学伦理委员会(23/180- 3922,2023年5月11日)审查并批准。本杂志总编辑可应要求提供一份书面同意书副本。
Prognostic impact of tumor location after abdominoperineal resection of rectal cancer: A single-center propensity score matching analysis based on 1806 cases.
Background: Randomized controlled trials have revealed that abdominoperineal resection leads to inferior oncological outcomes compared with low anterior resection, especially regarding local recurrence rates (LRRs). While neoadjuvant chemoradiotherapy can lower LRRs, it is linked to potential short- and long-term radiation-induced adverse effects. Consequently, meticulous patient selection for neoadjuvant chemoradiotherapy is imperative to balance benefits and risks.
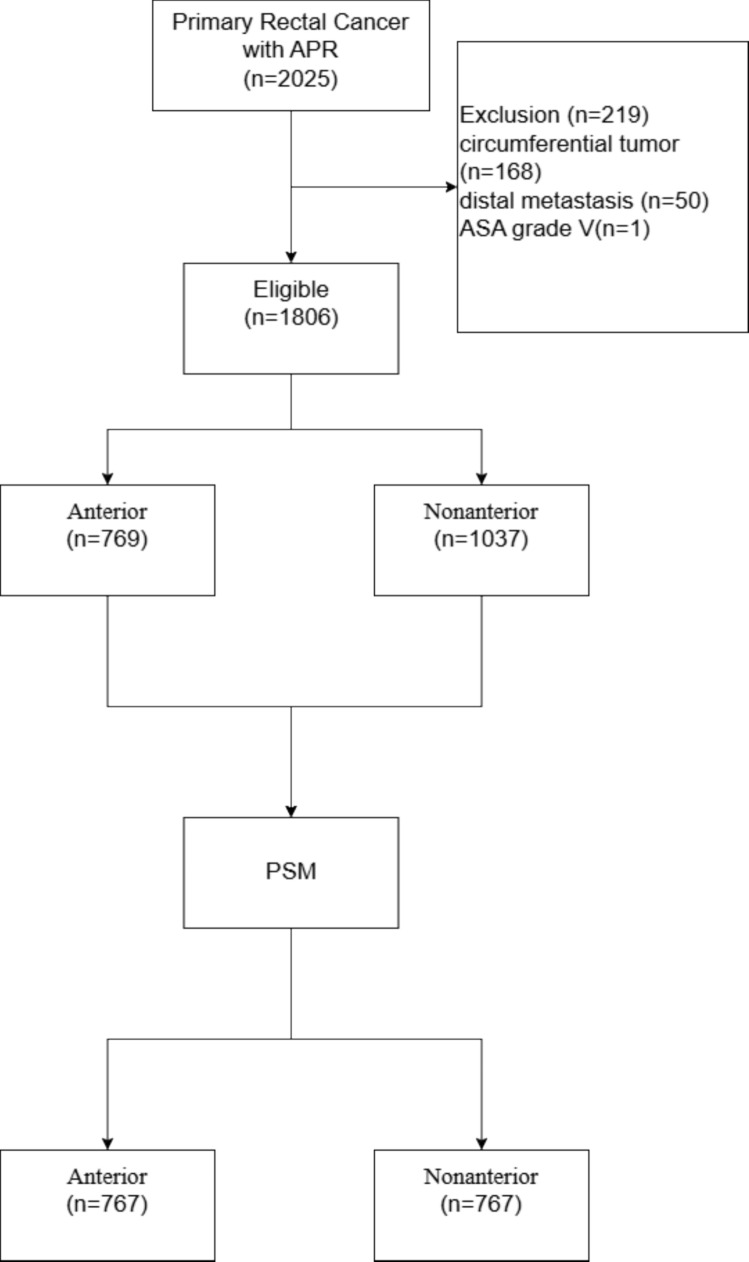
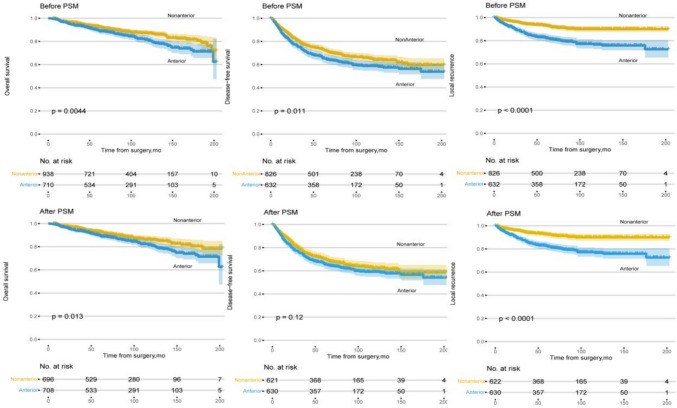
Methods: This research encompassed individuals with rectal cancer (RC) who underwent abdominoperineal resection (APR) from January 2006 to December 2017. The cohort was categorized into two cohorts on the basis of tumor location: the anterior cohort and the nonanterior cohort. Propensity score matching (PSM) was employed to mitigate selection bias, and this resulted in 767 patients in both cohorts. The primary endpoint assessed was survival without local recurrence (LR).
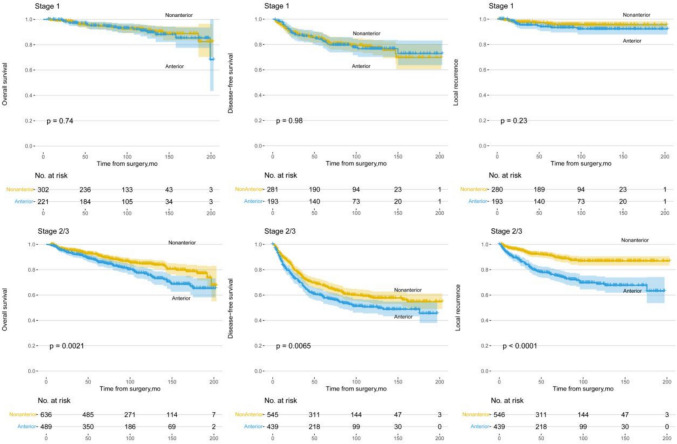
Results: Of the 2025 cases examined, 1806 were deemed eligible for inclusion. In the entire cohort, the incidence of LR was 9.9% (178/1806); the anterior cohort exhibited a higher rate of LR (15.2% versus 5.9%, p < 0.001). Multivariate examination revealed that anterior location was an independent risk factor (IRF) for LR (hazard ratio [HR] = 2.503, p < 0.001). In patients with stage II/III or T3/4, anterior location persisted as a predictor of increased LR. Neoadjuvant chemoradiotherapy for stage II and III tumors diminished the LR rate in anterior tumor locations (p = 0.017) but not in nonanterior locations (p = 0.390).
Conclusion: Anterior tumor location is an IRF for LR in RC patients. Tumor location can serve as a criterion for patient selection in neoadjuvant chemoradiotherapy.
Trial registration: The studies involving human participants were reviewed and approved by the National Cancer Center's Institute Research Medical Ethics Committee (23/180-3922, 11 May 2023). A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
期刊介绍:
Techniques in Coloproctology is an international journal fully devoted to diagnostic and operative procedures carried out in the management of colorectal diseases. Imaging, clinical physiology, laparoscopy, open abdominal surgery and proctoperineology are the main topics covered by the journal. Reviews, original articles, technical notes and short communications with many detailed illustrations render this publication indispensable for coloproctologists and related specialists. Both surgeons and gastroenterologists are represented on the distinguished Editorial Board, together with pathologists, radiologists and basic scientists from all over the world. The journal is strongly recommended to those who wish to be updated on recent developments in the field, and improve the standards of their work.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1965 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted. Reports of animal experiments must state that the Principles of Laboratory Animal Care (NIH publication no. 86-23 revised 1985) were followed as were applicable national laws (e.g. the current version of the German Law on the Protection of Animals). The Editor-in-Chief reserves the right to reject manuscripts that do not comply with the above-mentioned requirements. Authors will be held responsible for false statements or for failure to fulfill such requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


