Marie Juul Ornstrup, Agnethe Berglund, Mads Agerbæk, Claus Højbjerg Gravholt
{"title":"丹麦睾丸癌队列中预先存在的发病率模式:超越睾丸发育不良综合征假说的见解。","authors":"Marie Juul Ornstrup, Agnethe Berglund, Mads Agerbæk, Claus Højbjerg Gravholt","doi":"10.1093/hropen/hoaf021","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Do men diagnosed with testicular cancer (TC) exhibit increased pre-existing morbidity compared to matched controls?</p><p><strong>Summary answer: </strong>Men with TC had a significantly higher risk of hospital contacts and medicinal use prior to diagnosis compared to controls, reflecting excess morbidity across multiple health domains.</p><p><strong>What is known already: </strong>The testicular dysgenesis syndrome hypothesis suggests that, e.g. cryptorchidism, poor semen quality, and TC are all symptoms of a fetal gonadal dysgenesis. The association of TC with broader pre-existing morbidity remains unclear.</p><p><strong>Study design size duration: </strong>This retrospective, national, registry-based cohort study included 1952 TC patients, identified via the nationwide prospective clinical Danish Testicular Cancer (DATECA) database from 1 January 2013 to 28 February 2019, as well as 19 431 controls.</p><p><strong>Participants/materials setting methods: </strong>TC patients were matched with up to 10 randomly selected age-matched males from the background population. None of the controls were at any time registered in the DATECA database or with a TC diagnosis in either The Danish National Patient Register or The National Cancer Register. Hospital contact data and medication prescriptions were evaluated using national registries, categorized by the International Classification of Diseases, 8th edition (ICD-8) prior to 1993 and 10th edition (ICD-10) from 1993 onward, and the Anatomical Therapeutic Chemical (ATC) Classification, using data from birth until TC diagnosis. Negative binomial regression was used to compare 'Number of hospital contacts' within each ICD chapter for TC patients versus controls, and stratified Cox regression was used to compare 'time to first medicinal prescription' within each ATC-group.</p><p><strong>Main results and the role of chance: </strong>Prior to the TC diagnosis, the overall risk of hospital contacts was higher among TC patients than controls (incidence rate ratio (IRR)=1.18, CI: 1.13-1.25). IRRs were significantly increased in 11/18 chapters of the ICD-10, including cryptorchism (IRR = 3.24, CI: 2.31-4.52), indeterminate sex (IRR = 13.1, CI: 2.4-70.5), and infertility (IRR = 1.45, CI 1.08-2.01), and there were increased risks of respiratory, digestive, musculoskeletal, and nervous system diseases.The overall risk of being prescribed any medication was also increased among TC patients before their diagnosis (hazard ratio (HR)=1.28, CI: 1.21-1.34) compared to controls. HRs were significantly increased in 8/14 chapters of the ATC Classification, including the genito-urinary, respiratory, alimentary, musculoskeletal, and nervous system chapters. Risk of androgen prescriptions was not increased, whereas risks of prescription of gonadotropins (HR = 2.90, CI: 1.38-6.08) and medications related to erectile dysfunction (HR = 1.21, CI: 1.00-1.45) were.</p><p><strong>Limitations reasons for caution: </strong>The study is limited by the absence of clinical data, and thus there was no validation of diagnosis codes or prescription indications. However, the Danish national registries are generally recognized as high-quality data sources.</p><p><strong>Wider implications of the findings: </strong>The observed excess morbidity burden challenges the perception that TC males are largely healthy prior to their cancer diagnosis. The morbidity pattern reveals an increased risk of a wide variety of diseases, extending beyond those explained by the TDS hypothesis. These findings underpin that health personnel should be more vigilant regarding the presence of undiagnosed comorbidities and highlight the need for further research into potential shared etiological factors.</p><p><strong>Study funding/competing interests: </strong>The study was supported by grants from Aarhus University Hospital Research Fund and Health Research Foundation of Central Denmark Region (Grant number A3488). M.J.O. is an unpaid Medical Specialist Committee member of The Danish Patient Association for Adrenal insufficiency (Addison Foreningen). C.H.G. has received honoraria from Novo Nordisk, Sandoz, and Merck for talks presented on Turner syndrome. The remaining authors have nothing to disclose.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 2","pages":"hoaf021"},"PeriodicalIF":11.1000,"publicationDate":"2025-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12073984/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pre-existing morbidity pattern in a Danish testicular cancer cohort: insights beyond the testicular dysgenesis syndrome hypothesis.\",\"authors\":\"Marie Juul Ornstrup, Agnethe Berglund, Mads Agerbæk, Claus Højbjerg Gravholt\",\"doi\":\"10.1093/hropen/hoaf021\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study question: </strong>Do men diagnosed with testicular cancer (TC) exhibit increased pre-existing morbidity compared to matched controls?</p><p><strong>Summary answer: </strong>Men with TC had a significantly higher risk of hospital contacts and medicinal use prior to diagnosis compared to controls, reflecting excess morbidity across multiple health domains.</p><p><strong>What is known already: </strong>The testicular dysgenesis syndrome hypothesis suggests that, e.g. cryptorchidism, poor semen quality, and TC are all symptoms of a fetal gonadal dysgenesis. The association of TC with broader pre-existing morbidity remains unclear.</p><p><strong>Study design size duration: </strong>This retrospective, national, registry-based cohort study included 1952 TC patients, identified via the nationwide prospective clinical Danish Testicular Cancer (DATECA) database from 1 January 2013 to 28 February 2019, as well as 19 431 controls.</p><p><strong>Participants/materials setting methods: </strong>TC patients were matched with up to 10 randomly selected age-matched males from the background population. None of the controls were at any time registered in the DATECA database or with a TC diagnosis in either The Danish National Patient Register or The National Cancer Register. Hospital contact data and medication prescriptions were evaluated using national registries, categorized by the International Classification of Diseases, 8th edition (ICD-8) prior to 1993 and 10th edition (ICD-10) from 1993 onward, and the Anatomical Therapeutic Chemical (ATC) Classification, using data from birth until TC diagnosis. Negative binomial regression was used to compare 'Number of hospital contacts' within each ICD chapter for TC patients versus controls, and stratified Cox regression was used to compare 'time to first medicinal prescription' within each ATC-group.</p><p><strong>Main results and the role of chance: </strong>Prior to the TC diagnosis, the overall risk of hospital contacts was higher among TC patients than controls (incidence rate ratio (IRR)=1.18, CI: 1.13-1.25). IRRs were significantly increased in 11/18 chapters of the ICD-10, including cryptorchism (IRR = 3.24, CI: 2.31-4.52), indeterminate sex (IRR = 13.1, CI: 2.4-70.5), and infertility (IRR = 1.45, CI 1.08-2.01), and there were increased risks of respiratory, digestive, musculoskeletal, and nervous system diseases.The overall risk of being prescribed any medication was also increased among TC patients before their diagnosis (hazard ratio (HR)=1.28, CI: 1.21-1.34) compared to controls. HRs were significantly increased in 8/14 chapters of the ATC Classification, including the genito-urinary, respiratory, alimentary, musculoskeletal, and nervous system chapters. Risk of androgen prescriptions was not increased, whereas risks of prescription of gonadotropins (HR = 2.90, CI: 1.38-6.08) and medications related to erectile dysfunction (HR = 1.21, CI: 1.00-1.45) were.</p><p><strong>Limitations reasons for caution: </strong>The study is limited by the absence of clinical data, and thus there was no validation of diagnosis codes or prescription indications. However, the Danish national registries are generally recognized as high-quality data sources.</p><p><strong>Wider implications of the findings: </strong>The observed excess morbidity burden challenges the perception that TC males are largely healthy prior to their cancer diagnosis. The morbidity pattern reveals an increased risk of a wide variety of diseases, extending beyond those explained by the TDS hypothesis. These findings underpin that health personnel should be more vigilant regarding the presence of undiagnosed comorbidities and highlight the need for further research into potential shared etiological factors.</p><p><strong>Study funding/competing interests: </strong>The study was supported by grants from Aarhus University Hospital Research Fund and Health Research Foundation of Central Denmark Region (Grant number A3488). M.J.O. is an unpaid Medical Specialist Committee member of The Danish Patient Association for Adrenal insufficiency (Addison Foreningen). C.H.G. has received honoraria from Novo Nordisk, Sandoz, and Merck for talks presented on Turner syndrome. The remaining authors have nothing to disclose.</p><p><strong>Trial registration number: </strong>N/A.</p>\",\"PeriodicalId\":73264,\"journal\":{\"name\":\"Human reproduction open\",\"volume\":\"2025 2\",\"pages\":\"hoaf021\"},\"PeriodicalIF\":11.1000,\"publicationDate\":\"2025-04-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12073984/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human reproduction open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/hropen/hoaf021\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Pre-existing morbidity pattern in a Danish testicular cancer cohort: insights beyond the testicular dysgenesis syndrome hypothesis.
Study question: Do men diagnosed with testicular cancer (TC) exhibit increased pre-existing morbidity compared to matched controls?
Summary answer: Men with TC had a significantly higher risk of hospital contacts and medicinal use prior to diagnosis compared to controls, reflecting excess morbidity across multiple health domains.
What is known already: The testicular dysgenesis syndrome hypothesis suggests that, e.g. cryptorchidism, poor semen quality, and TC are all symptoms of a fetal gonadal dysgenesis. The association of TC with broader pre-existing morbidity remains unclear.
Study design size duration: This retrospective, national, registry-based cohort study included 1952 TC patients, identified via the nationwide prospective clinical Danish Testicular Cancer (DATECA) database from 1 January 2013 to 28 February 2019, as well as 19 431 controls.
Participants/materials setting methods: TC patients were matched with up to 10 randomly selected age-matched males from the background population. None of the controls were at any time registered in the DATECA database or with a TC diagnosis in either The Danish National Patient Register or The National Cancer Register. Hospital contact data and medication prescriptions were evaluated using national registries, categorized by the International Classification of Diseases, 8th edition (ICD-8) prior to 1993 and 10th edition (ICD-10) from 1993 onward, and the Anatomical Therapeutic Chemical (ATC) Classification, using data from birth until TC diagnosis. Negative binomial regression was used to compare 'Number of hospital contacts' within each ICD chapter for TC patients versus controls, and stratified Cox regression was used to compare 'time to first medicinal prescription' within each ATC-group.
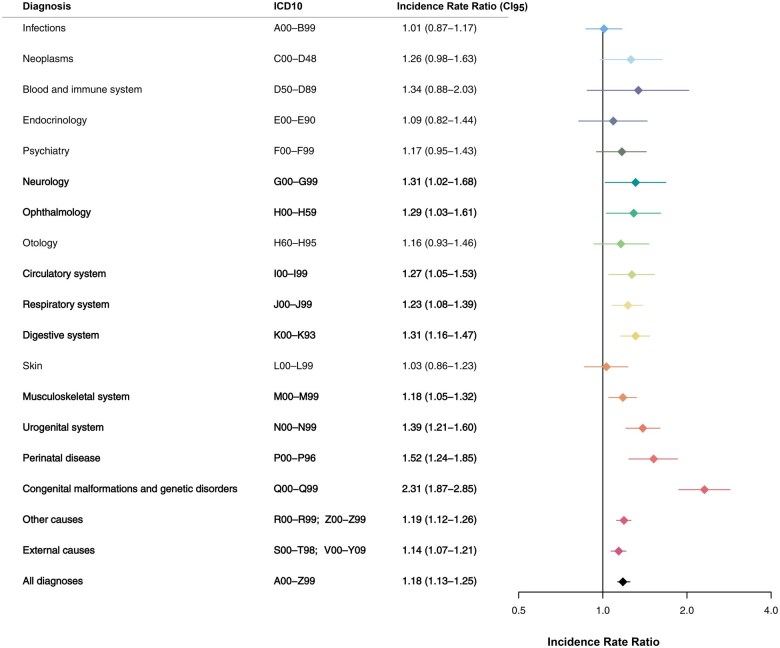
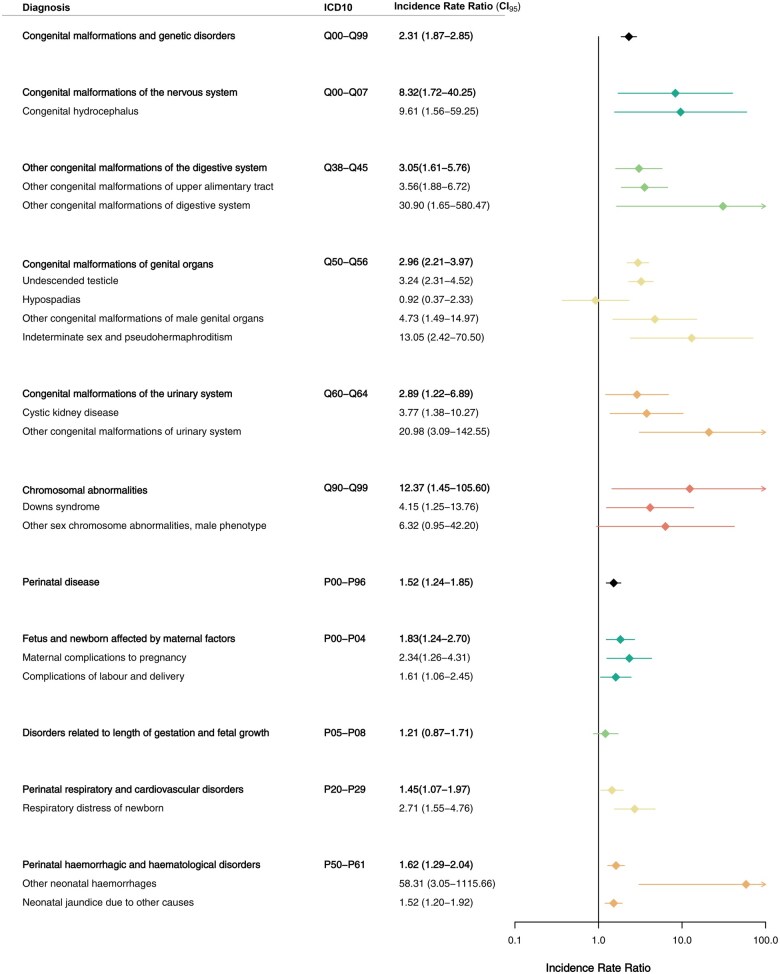
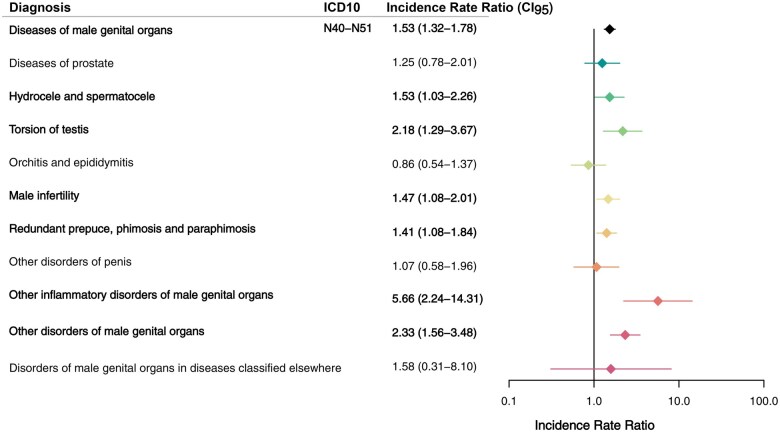
Main results and the role of chance: Prior to the TC diagnosis, the overall risk of hospital contacts was higher among TC patients than controls (incidence rate ratio (IRR)=1.18, CI: 1.13-1.25). IRRs were significantly increased in 11/18 chapters of the ICD-10, including cryptorchism (IRR = 3.24, CI: 2.31-4.52), indeterminate sex (IRR = 13.1, CI: 2.4-70.5), and infertility (IRR = 1.45, CI 1.08-2.01), and there were increased risks of respiratory, digestive, musculoskeletal, and nervous system diseases.The overall risk of being prescribed any medication was also increased among TC patients before their diagnosis (hazard ratio (HR)=1.28, CI: 1.21-1.34) compared to controls. HRs were significantly increased in 8/14 chapters of the ATC Classification, including the genito-urinary, respiratory, alimentary, musculoskeletal, and nervous system chapters. Risk of androgen prescriptions was not increased, whereas risks of prescription of gonadotropins (HR = 2.90, CI: 1.38-6.08) and medications related to erectile dysfunction (HR = 1.21, CI: 1.00-1.45) were.
Limitations reasons for caution: The study is limited by the absence of clinical data, and thus there was no validation of diagnosis codes or prescription indications. However, the Danish national registries are generally recognized as high-quality data sources.
Wider implications of the findings: The observed excess morbidity burden challenges the perception that TC males are largely healthy prior to their cancer diagnosis. The morbidity pattern reveals an increased risk of a wide variety of diseases, extending beyond those explained by the TDS hypothesis. These findings underpin that health personnel should be more vigilant regarding the presence of undiagnosed comorbidities and highlight the need for further research into potential shared etiological factors.
Study funding/competing interests: The study was supported by grants from Aarhus University Hospital Research Fund and Health Research Foundation of Central Denmark Region (Grant number A3488). M.J.O. is an unpaid Medical Specialist Committee member of The Danish Patient Association for Adrenal insufficiency (Addison Foreningen). C.H.G. has received honoraria from Novo Nordisk, Sandoz, and Merck for talks presented on Turner syndrome. The remaining authors have nothing to disclose.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


