Guglielmo Stabile, Chiara Ripepi, Giuseppe Ricci, Luigi Nappi, Giulia Oletto, Manuela Ludovisi, Giovanni Scambia, Matteo Bruno
{"title":"真空抽吸或子宫腔扩张刮除后子宫穿孔后输卵管嵌顿或肠套叠的诊断、处理和结局:系统的文献综述。","authors":"Guglielmo Stabile, Chiara Ripepi, Giuseppe Ricci, Luigi Nappi, Giulia Oletto, Manuela Ludovisi, Giovanni Scambia, Matteo Bruno","doi":"10.52054/FVVO.2024.12791","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dilation and curettage and vacuum aspiration are frequently performed gynaecological procedures used to treat uterine pathology. This procedure carries a risk of uterine perforation, which can lead to injury of abdominal organs and, rarely, to fallopian tubes.</p><p><strong>Objectives: </strong>To evaluate symptoms and diagnostic signs and to propose the most appropriate management for the intussusception and incarceration of fallopian tubes following uterine aspiration and curettage.</p><p><strong>Methods: </strong>We screened three major databases (Medline, Scopus, Google Scholar) from 2000 to May 2024. Our review examined tubal incarceration, causes, management, symptoms, parity, diagnosis timelines, visceral injury, and surgical complications. The methodological quality of the included studies was assessed using the JBI Critical Appraisal Checklist for case reports.</p><p><strong>Main outcome measures: </strong>Diagnostic methods, complications and management of tubal incarceration following uterine perforation.</p><p><strong>Results: </strong>We identified 24 papers, all of which were case reports or case series. In our analysis, tubal incarceration was observed in 25 of 26 cases (96.2%) and in 2 of which (7.7%) it was associated with the entrapment of the infundibulopelvic ligament. In 1 of 26 cases (3.8%) intussusception of the fallopian tube was observed. The most frequently manifested symptoms were abdominopelvic pain, vaginal bleeding, vaginal discharge and amenorrhoea. The mean time to diagnosis was 15.4 months, with transvaginal ultrasound being the primary diagnostic tool, followed by hysteroscopy and diagnostic laparoscopy.</p><p><strong>Conclusions: </strong>Diagnosing this condition should involve a detailed medical history, a comprehensive clinical examination, and imaging evaluations. If instrumental investigations are negative but suspicion remains, hysteroscopy and/or laparoscopy may be necessary.</p><p><strong>What is new?: </strong>Tubal incarceration complicating uterine perforation can be managed using hysteroscopy and laparoscopy.</p>","PeriodicalId":46400,"journal":{"name":"Facts Views and Vision in ObGyn","volume":"17 1","pages":"39-49"},"PeriodicalIF":1.4000,"publicationDate":"2025-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12042149/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnosis, management and outcomes of incarceration or intussusception of Fallopian tubes following uterine perforation after vacuum aspiration or dilatation and curettage of the uterine cavity: a systematic review of the literature.\",\"authors\":\"Guglielmo Stabile, Chiara Ripepi, Giuseppe Ricci, Luigi Nappi, Giulia Oletto, Manuela Ludovisi, Giovanni Scambia, Matteo Bruno\",\"doi\":\"10.52054/FVVO.2024.12791\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Dilation and curettage and vacuum aspiration are frequently performed gynaecological procedures used to treat uterine pathology. This procedure carries a risk of uterine perforation, which can lead to injury of abdominal organs and, rarely, to fallopian tubes.</p><p><strong>Objectives: </strong>To evaluate symptoms and diagnostic signs and to propose the most appropriate management for the intussusception and incarceration of fallopian tubes following uterine aspiration and curettage.</p><p><strong>Methods: </strong>We screened three major databases (Medline, Scopus, Google Scholar) from 2000 to May 2024. Our review examined tubal incarceration, causes, management, symptoms, parity, diagnosis timelines, visceral injury, and surgical complications. The methodological quality of the included studies was assessed using the JBI Critical Appraisal Checklist for case reports.</p><p><strong>Main outcome measures: </strong>Diagnostic methods, complications and management of tubal incarceration following uterine perforation.</p><p><strong>Results: </strong>We identified 24 papers, all of which were case reports or case series. In our analysis, tubal incarceration was observed in 25 of 26 cases (96.2%) and in 2 of which (7.7%) it was associated with the entrapment of the infundibulopelvic ligament. In 1 of 26 cases (3.8%) intussusception of the fallopian tube was observed. The most frequently manifested symptoms were abdominopelvic pain, vaginal bleeding, vaginal discharge and amenorrhoea. The mean time to diagnosis was 15.4 months, with transvaginal ultrasound being the primary diagnostic tool, followed by hysteroscopy and diagnostic laparoscopy.</p><p><strong>Conclusions: </strong>Diagnosing this condition should involve a detailed medical history, a comprehensive clinical examination, and imaging evaluations. If instrumental investigations are negative but suspicion remains, hysteroscopy and/or laparoscopy may be necessary.</p><p><strong>What is new?: </strong>Tubal incarceration complicating uterine perforation can be managed using hysteroscopy and laparoscopy.</p>\",\"PeriodicalId\":46400,\"journal\":{\"name\":\"Facts Views and Vision in ObGyn\",\"volume\":\"17 1\",\"pages\":\"39-49\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12042149/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Facts Views and Vision in ObGyn\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.52054/FVVO.2024.12791\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Facts Views and Vision in ObGyn","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.52054/FVVO.2024.12791","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Diagnosis, management and outcomes of incarceration or intussusception of Fallopian tubes following uterine perforation after vacuum aspiration or dilatation and curettage of the uterine cavity: a systematic review of the literature.
Background: Dilation and curettage and vacuum aspiration are frequently performed gynaecological procedures used to treat uterine pathology. This procedure carries a risk of uterine perforation, which can lead to injury of abdominal organs and, rarely, to fallopian tubes.
Objectives: To evaluate symptoms and diagnostic signs and to propose the most appropriate management for the intussusception and incarceration of fallopian tubes following uterine aspiration and curettage.
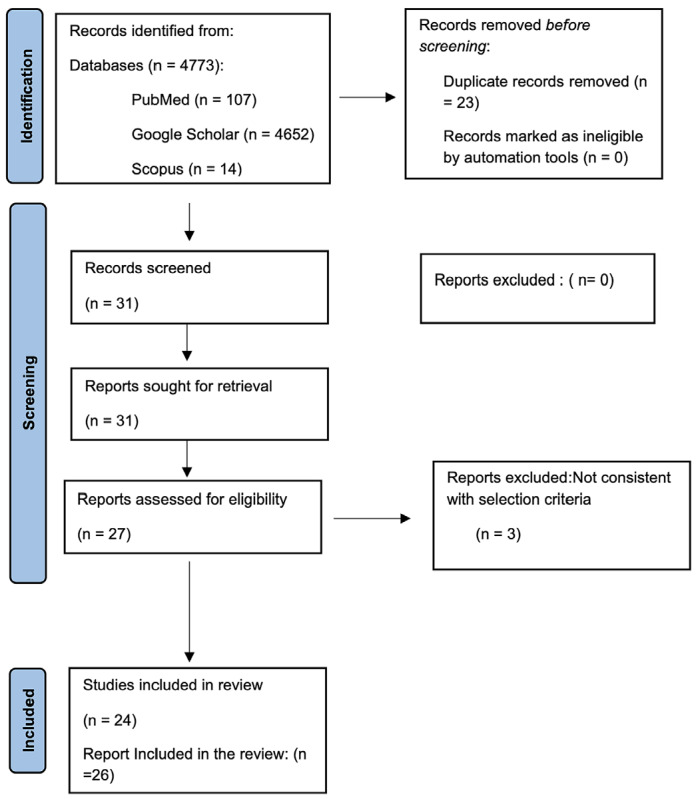
Methods: We screened three major databases (Medline, Scopus, Google Scholar) from 2000 to May 2024. Our review examined tubal incarceration, causes, management, symptoms, parity, diagnosis timelines, visceral injury, and surgical complications. The methodological quality of the included studies was assessed using the JBI Critical Appraisal Checklist for case reports.
Main outcome measures: Diagnostic methods, complications and management of tubal incarceration following uterine perforation.
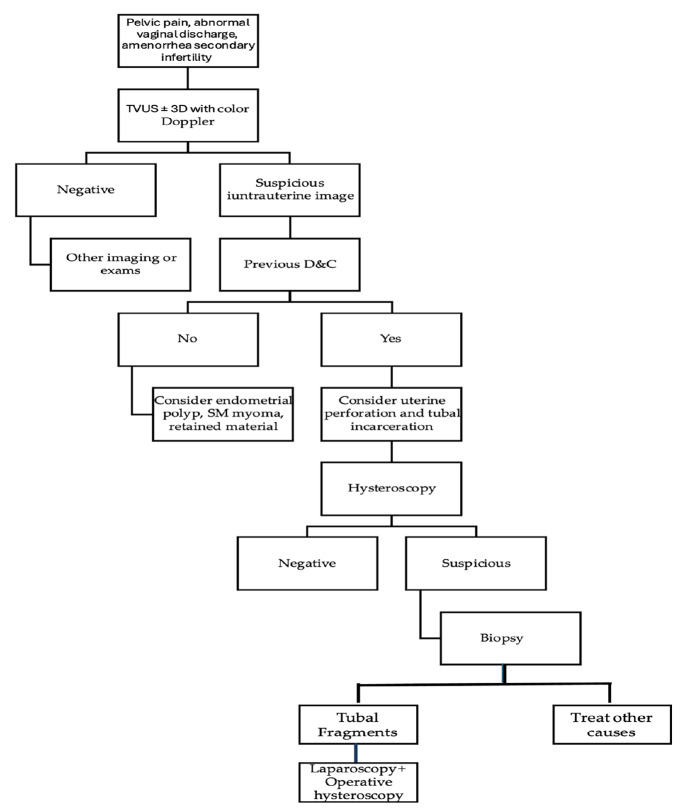
Results: We identified 24 papers, all of which were case reports or case series. In our analysis, tubal incarceration was observed in 25 of 26 cases (96.2%) and in 2 of which (7.7%) it was associated with the entrapment of the infundibulopelvic ligament. In 1 of 26 cases (3.8%) intussusception of the fallopian tube was observed. The most frequently manifested symptoms were abdominopelvic pain, vaginal bleeding, vaginal discharge and amenorrhoea. The mean time to diagnosis was 15.4 months, with transvaginal ultrasound being the primary diagnostic tool, followed by hysteroscopy and diagnostic laparoscopy.
Conclusions: Diagnosing this condition should involve a detailed medical history, a comprehensive clinical examination, and imaging evaluations. If instrumental investigations are negative but suspicion remains, hysteroscopy and/or laparoscopy may be necessary.
What is new?: Tubal incarceration complicating uterine perforation can be managed using hysteroscopy and laparoscopy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


