Andrew Richard Coggins, Vinh Dat David Nguyen, Leonardo Pasalic, Murari Ramesh, Kush Wangoo
{"title":"急诊创伤患者即时粘弹性止血试验的应用","authors":"Andrew Richard Coggins, Vinh Dat David Nguyen, Leonardo Pasalic, Murari Ramesh, Kush Wangoo","doi":"10.1186/s13049-025-01388-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Traumatic haemorrhage often requires initiation of a massive haemorrhage protocol (MHP). The primary aim of this exploratory Emergency Department (ED) study was to examine the utility of point of care Viscoelastic Haemostatic Assays (VHA) in terms of accuracy. The primary outcome was prediction of the need for massive transfusion (MT) at 24-hours.</p><p><strong>Methods: </strong>Prospective observational study of consecutive trauma patients investigated with reported using STARD guidelines. Patients in an Australian ED setting < 1-hour from triage enrolled in a three-year window. The point-of-care device used was a TEG6s™ (Haemonetics, Braintree, MA, USA). The primary outcome was accuracy VHA testing for predicting MT delivery at 24-hours (an internationally recognised of massive transfusion was used). Other trauma outcomes such as product transfusion, injury severity score (ISS) and demographics were recorded. For analysis of accuracy the cohort was divided into VHA-normal (n = 44) and VHA-abnormal (n = 70) binary groups. Secondary outcomes included utility of TEG6s™ individual components and accuracy of VHA when combined with validated MHP decision scores.</p><p><strong>Results: </strong>Among eligible cases (n = 114) in-patient mortality was 7.0% with 91.2% receiving transfusion. Presence of (any) abnormal VHA result provided a 73.6% (95%CI 59.7-84.7) sensitivity and 49.3% (95%CI 36.1-62.3) specificity for predicting MT. Citrated Functional Fibrinogen (CFF) component had a higher performance for MT \"rule-in\" specificity (86.9%). When VHA was combined with validated MHP decision scores performance was increased. For example, normal VHA with Trauma Associated Severe Haemorrhage score < 8.5 was observed to yield a sensitivity of 96.2% for MT requirement rule-out. Further studies should examine if VHA test parameters can be added or (replace INR) in the existing clinical scores used to make decisions about transfusion in ED patients.</p><p><strong>Conclusion: </strong>The standalone performance of early VHA testing in the ED setting was insufficient to reliably for predict a need for massive transfusion.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"68"},"PeriodicalIF":3.1000,"publicationDate":"2025-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12023681/pdf/","citationCount":"0","resultStr":"{\"title\":\"Utility of point of care viscoelastic haemostatic assays for trauma patients in the emergency department.\",\"authors\":\"Andrew Richard Coggins, Vinh Dat David Nguyen, Leonardo Pasalic, Murari Ramesh, Kush Wangoo\",\"doi\":\"10.1186/s13049-025-01388-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Traumatic haemorrhage often requires initiation of a massive haemorrhage protocol (MHP). The primary aim of this exploratory Emergency Department (ED) study was to examine the utility of point of care Viscoelastic Haemostatic Assays (VHA) in terms of accuracy. The primary outcome was prediction of the need for massive transfusion (MT) at 24-hours.</p><p><strong>Methods: </strong>Prospective observational study of consecutive trauma patients investigated with reported using STARD guidelines. Patients in an Australian ED setting < 1-hour from triage enrolled in a three-year window. The point-of-care device used was a TEG6s™ (Haemonetics, Braintree, MA, USA). The primary outcome was accuracy VHA testing for predicting MT delivery at 24-hours (an internationally recognised of massive transfusion was used). Other trauma outcomes such as product transfusion, injury severity score (ISS) and demographics were recorded. For analysis of accuracy the cohort was divided into VHA-normal (n = 44) and VHA-abnormal (n = 70) binary groups. Secondary outcomes included utility of TEG6s™ individual components and accuracy of VHA when combined with validated MHP decision scores.</p><p><strong>Results: </strong>Among eligible cases (n = 114) in-patient mortality was 7.0% with 91.2% receiving transfusion. Presence of (any) abnormal VHA result provided a 73.6% (95%CI 59.7-84.7) sensitivity and 49.3% (95%CI 36.1-62.3) specificity for predicting MT. Citrated Functional Fibrinogen (CFF) component had a higher performance for MT \\\"rule-in\\\" specificity (86.9%). When VHA was combined with validated MHP decision scores performance was increased. For example, normal VHA with Trauma Associated Severe Haemorrhage score < 8.5 was observed to yield a sensitivity of 96.2% for MT requirement rule-out. Further studies should examine if VHA test parameters can be added or (replace INR) in the existing clinical scores used to make decisions about transfusion in ED patients.</p><p><strong>Conclusion: </strong>The standalone performance of early VHA testing in the ED setting was insufficient to reliably for predict a need for massive transfusion.</p>\",\"PeriodicalId\":49292,\"journal\":{\"name\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"volume\":\"33 1\",\"pages\":\"68\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-04-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12023681/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13049-025-01388-1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01388-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Utility of point of care viscoelastic haemostatic assays for trauma patients in the emergency department.
Background and objectives: Traumatic haemorrhage often requires initiation of a massive haemorrhage protocol (MHP). The primary aim of this exploratory Emergency Department (ED) study was to examine the utility of point of care Viscoelastic Haemostatic Assays (VHA) in terms of accuracy. The primary outcome was prediction of the need for massive transfusion (MT) at 24-hours.
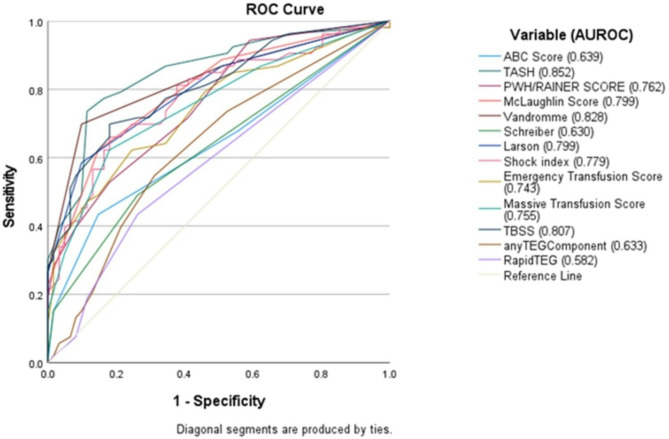
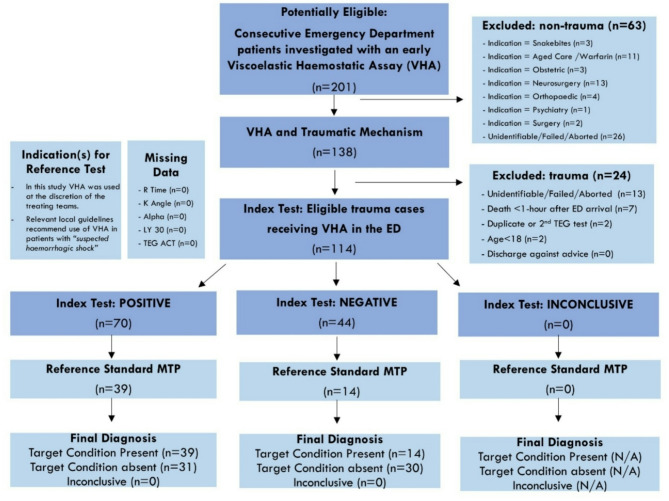
Methods: Prospective observational study of consecutive trauma patients investigated with reported using STARD guidelines. Patients in an Australian ED setting < 1-hour from triage enrolled in a three-year window. The point-of-care device used was a TEG6s™ (Haemonetics, Braintree, MA, USA). The primary outcome was accuracy VHA testing for predicting MT delivery at 24-hours (an internationally recognised of massive transfusion was used). Other trauma outcomes such as product transfusion, injury severity score (ISS) and demographics were recorded. For analysis of accuracy the cohort was divided into VHA-normal (n = 44) and VHA-abnormal (n = 70) binary groups. Secondary outcomes included utility of TEG6s™ individual components and accuracy of VHA when combined with validated MHP decision scores.
Results: Among eligible cases (n = 114) in-patient mortality was 7.0% with 91.2% receiving transfusion. Presence of (any) abnormal VHA result provided a 73.6% (95%CI 59.7-84.7) sensitivity and 49.3% (95%CI 36.1-62.3) specificity for predicting MT. Citrated Functional Fibrinogen (CFF) component had a higher performance for MT "rule-in" specificity (86.9%). When VHA was combined with validated MHP decision scores performance was increased. For example, normal VHA with Trauma Associated Severe Haemorrhage score < 8.5 was observed to yield a sensitivity of 96.2% for MT requirement rule-out. Further studies should examine if VHA test parameters can be added or (replace INR) in the existing clinical scores used to make decisions about transfusion in ED patients.
Conclusion: The standalone performance of early VHA testing in the ED setting was insufficient to reliably for predict a need for massive transfusion.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


