Shuoyan An, Wuqiang Che, Yanxiang Gao, Xiaoyan Duo, Xingliang Li, Jiahui Li
{"title":"全血细胞计数指标对合并冠心病和慢性肾病患者短期死亡率的预测价值","authors":"Shuoyan An, Wuqiang Che, Yanxiang Gao, Xiaoyan Duo, Xingliang Li, Jiahui Li","doi":"10.2147/IJNRD.S508019","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Patients with chronic kidney disease (CKD) and coronary artery disease (CAD) had a poor prognosis. Indicators derived from complete blood count (CBC), like neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), monocyte-lymphocyte ratio (MLR), Systematic Inflammation Response Index (SIRI), systemic immune-inflammation index (SII) and Pan-Immune-Inflammation Value (PIV) had prognostic significance. But which one performed best in patients with CKD and CAD was still unclear.</p><p><strong>Methods: </strong>CKD Patients with CAD admitted to ICU were retrospectively included. Patients with sepsis, connective tissue disease, tumor and receiving glucocorticoids were excluded. The primary endpoints encompassed in-hospital mortality and 30-day mortality.</p><p><strong>Results: </strong>The study comprised 694 participants, with 60 patients died during hospitalization, and another 15 died in 30-day follow-up period. Both the admission level and maximal level of CBC-derived indicators were higher in the deceased group. ROC curve analysis demonstrated that maximal NLR had the highest AUCs - 0.795 for in-hospital mortality and 0.754 for 30-day mortality prediction. Furthermore, Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) analyses further confirmed that adding maximal NLR to the base model, which included traditional risk factors, significantly improved both NRI and IDI (p < 0.05 for both).</p><p><strong>Conclusion: </strong>The maximum of NLR was with the best predictive value for in-hospital mortality and 30-day mortality in ICU patients with CAD and CKD. Predicting prognosis based on dynamic changes of NLR is more worthy of attention.</p>","PeriodicalId":14181,"journal":{"name":"International Journal of Nephrology and Renovascular Disease","volume":"18 ","pages":"113-122"},"PeriodicalIF":2.5000,"publicationDate":"2025-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12009582/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictive Value of Complete Blood Count Indicators for Short-Term Mortality in Patients with Combined Coronary Artery Disease and Chronic Kidney Disease.\",\"authors\":\"Shuoyan An, Wuqiang Che, Yanxiang Gao, Xiaoyan Duo, Xingliang Li, Jiahui Li\",\"doi\":\"10.2147/IJNRD.S508019\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Patients with chronic kidney disease (CKD) and coronary artery disease (CAD) had a poor prognosis. Indicators derived from complete blood count (CBC), like neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), monocyte-lymphocyte ratio (MLR), Systematic Inflammation Response Index (SIRI), systemic immune-inflammation index (SII) and Pan-Immune-Inflammation Value (PIV) had prognostic significance. But which one performed best in patients with CKD and CAD was still unclear.</p><p><strong>Methods: </strong>CKD Patients with CAD admitted to ICU were retrospectively included. Patients with sepsis, connective tissue disease, tumor and receiving glucocorticoids were excluded. The primary endpoints encompassed in-hospital mortality and 30-day mortality.</p><p><strong>Results: </strong>The study comprised 694 participants, with 60 patients died during hospitalization, and another 15 died in 30-day follow-up period. Both the admission level and maximal level of CBC-derived indicators were higher in the deceased group. ROC curve analysis demonstrated that maximal NLR had the highest AUCs - 0.795 for in-hospital mortality and 0.754 for 30-day mortality prediction. Furthermore, Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) analyses further confirmed that adding maximal NLR to the base model, which included traditional risk factors, significantly improved both NRI and IDI (p < 0.05 for both).</p><p><strong>Conclusion: </strong>The maximum of NLR was with the best predictive value for in-hospital mortality and 30-day mortality in ICU patients with CAD and CKD. Predicting prognosis based on dynamic changes of NLR is more worthy of attention.</p>\",\"PeriodicalId\":14181,\"journal\":{\"name\":\"International Journal of Nephrology and Renovascular Disease\",\"volume\":\"18 \",\"pages\":\"113-122\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-04-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12009582/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Nephrology and Renovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/IJNRD.S508019\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Nephrology and Renovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IJNRD.S508019","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Predictive Value of Complete Blood Count Indicators for Short-Term Mortality in Patients with Combined Coronary Artery Disease and Chronic Kidney Disease.
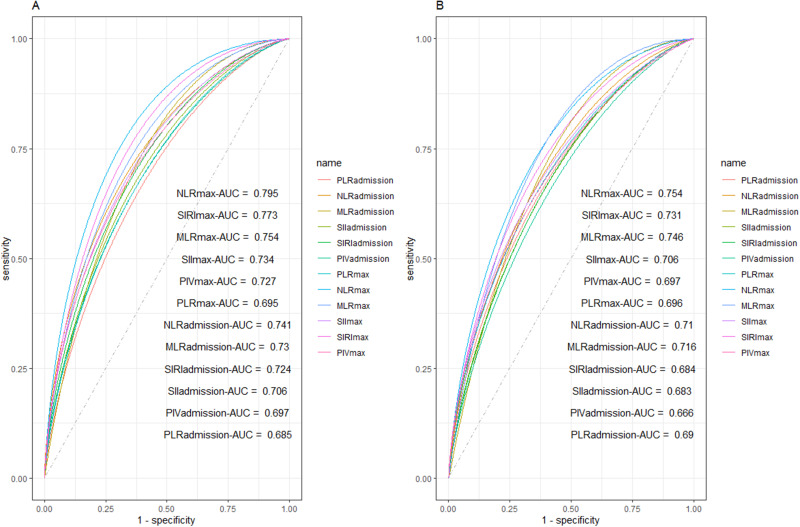
Objective: Patients with chronic kidney disease (CKD) and coronary artery disease (CAD) had a poor prognosis. Indicators derived from complete blood count (CBC), like neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), monocyte-lymphocyte ratio (MLR), Systematic Inflammation Response Index (SIRI), systemic immune-inflammation index (SII) and Pan-Immune-Inflammation Value (PIV) had prognostic significance. But which one performed best in patients with CKD and CAD was still unclear.
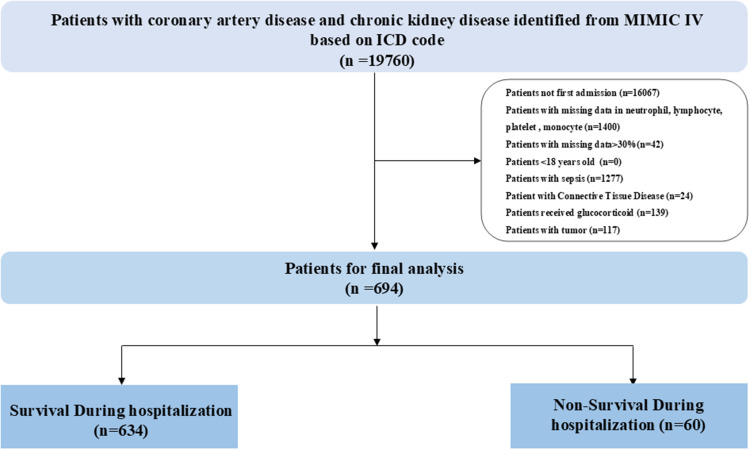
Methods: CKD Patients with CAD admitted to ICU were retrospectively included. Patients with sepsis, connective tissue disease, tumor and receiving glucocorticoids were excluded. The primary endpoints encompassed in-hospital mortality and 30-day mortality.
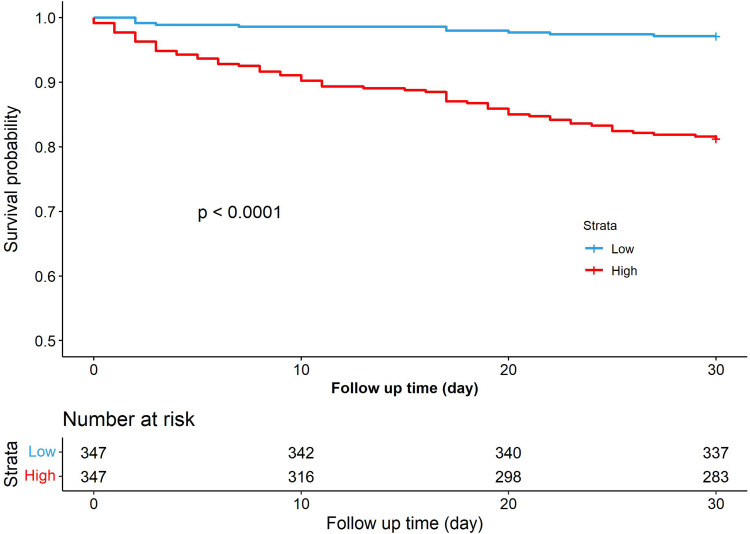
Results: The study comprised 694 participants, with 60 patients died during hospitalization, and another 15 died in 30-day follow-up period. Both the admission level and maximal level of CBC-derived indicators were higher in the deceased group. ROC curve analysis demonstrated that maximal NLR had the highest AUCs - 0.795 for in-hospital mortality and 0.754 for 30-day mortality prediction. Furthermore, Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) analyses further confirmed that adding maximal NLR to the base model, which included traditional risk factors, significantly improved both NRI and IDI (p < 0.05 for both).
Conclusion: The maximum of NLR was with the best predictive value for in-hospital mortality and 30-day mortality in ICU patients with CAD and CKD. Predicting prognosis based on dynamic changes of NLR is more worthy of attention.
期刊介绍:
International Journal of Nephrology and Renovascular Disease is an international, peer-reviewed, open-access journal focusing on the pathophysiology of the kidney and vascular supply. Epidemiology, screening, diagnosis, and treatment interventions are covered as well as basic science, biochemical and immunological studies. In particular, emphasis will be given to: -Chronic kidney disease- Complications of renovascular disease- Imaging techniques- Renal hypertension- Renal cancer- Treatment including pharmacological and transplantation- Dialysis and treatment of complications of dialysis and renal disease- Quality of Life- Patient satisfaction and preference- Health economic evaluations. The journal welcomes submitted papers covering original research, basic science, clinical studies, reviews & evaluations, guidelines, expert opinion and commentary, case reports and extended reports. The main focus of the journal will be to publish research and clinical results in humans but preclinical, animal and in vitro studies will be published where they shed light on disease processes and potential new therapies and interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


