{"title":"肝内胆管癌晚期淋巴结转移的定义:一项多中心研究。","authors":"Makoto Kurimoto, Tomoaki Yoh, Shinichi Nakanuma, Hiroaki Sugita, Hideaki Sueoka, Ikuo Nakamura, Seiko Hirono, Takamichi Ishii, Shintaro Yagi, Etsuro Hatano","doi":"10.1111/hepr.14196","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>There is no specific boundary for stratifying survival outcomes in patients with node-positive intrahepatic cholangiocarcinoma (ICC). This study aimed to propose advanced nodal status in ICC.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Data from patients with pathologically confirmed node-positive ICC who underwent liver resection (LR) with lymph node dissection (LND) from 2000 to 2020 at three tertiary centers were retrospectively analyzed. The boundaries of regions and the yield that stratified overall survival (OS) were evaluated. The lymph node (LN) regions were defined as follows: hepatoduodenal ligament, common hepatic artery, and peripancreatic area (HCP-area), gastrohepatic area (GH-area), and para-aortic area (A-area).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Eighty-four patients with node-positive ICC were enrolled in this study. The median numbers of retrieved LNs and involved LNs (ILNs) were 15 (range: 2–56) and 2 (range: 1–20), respectively. Most patients (96.5%) had ILNs in the HCP-area, whereas only 3 patients (3.5%) had ILNs in other areas without HCP-area involvement. OS of patients with LN metastasis confined to the HCP-area was better than for those beyond this area (median OS: 24.3 vs. 13.3 months, <i>p</i> = 0.047). The best cut-off number of ILNs to stratify OS was 4, and patients with 1–3 ILNs showed better OS than those with ≥ 4 ILNs (25.4 vs. 13.8 months, <i>p</i> = 0.006). Combining distribution and yield showed the best prognostic power compared to using either distribution or yield alone.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In patients with node-positive ICC, LN metastasis beyond the HCP-area or ≥ 4 ILNs can be proposed as advanced N disease.</p>\n </section>\n </div>","PeriodicalId":12987,"journal":{"name":"Hepatology Research","volume":"55 7","pages":"1038-1045"},"PeriodicalIF":3.4000,"publicationDate":"2025-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Defining advanced lymph node metastasis in intrahepatic cholangiocarcinoma: A multicenter study\",\"authors\":\"Makoto Kurimoto, Tomoaki Yoh, Shinichi Nakanuma, Hiroaki Sugita, Hideaki Sueoka, Ikuo Nakamura, Seiko Hirono, Takamichi Ishii, Shintaro Yagi, Etsuro Hatano\",\"doi\":\"10.1111/hepr.14196\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>There is no specific boundary for stratifying survival outcomes in patients with node-positive intrahepatic cholangiocarcinoma (ICC). This study aimed to propose advanced nodal status in ICC.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Data from patients with pathologically confirmed node-positive ICC who underwent liver resection (LR) with lymph node dissection (LND) from 2000 to 2020 at three tertiary centers were retrospectively analyzed. The boundaries of regions and the yield that stratified overall survival (OS) were evaluated. The lymph node (LN) regions were defined as follows: hepatoduodenal ligament, common hepatic artery, and peripancreatic area (HCP-area), gastrohepatic area (GH-area), and para-aortic area (A-area).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Eighty-four patients with node-positive ICC were enrolled in this study. The median numbers of retrieved LNs and involved LNs (ILNs) were 15 (range: 2–56) and 2 (range: 1–20), respectively. Most patients (96.5%) had ILNs in the HCP-area, whereas only 3 patients (3.5%) had ILNs in other areas without HCP-area involvement. OS of patients with LN metastasis confined to the HCP-area was better than for those beyond this area (median OS: 24.3 vs. 13.3 months, <i>p</i> = 0.047). The best cut-off number of ILNs to stratify OS was 4, and patients with 1–3 ILNs showed better OS than those with ≥ 4 ILNs (25.4 vs. 13.8 months, <i>p</i> = 0.006). Combining distribution and yield showed the best prognostic power compared to using either distribution or yield alone.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In patients with node-positive ICC, LN metastasis beyond the HCP-area or ≥ 4 ILNs can be proposed as advanced N disease.</p>\\n </section>\\n </div>\",\"PeriodicalId\":12987,\"journal\":{\"name\":\"Hepatology Research\",\"volume\":\"55 7\",\"pages\":\"1038-1045\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-04-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hepatology Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/hepr.14196\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatology Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/hepr.14196","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:对于淋巴结阳性肝内胆管癌(ICC)患者的生存结局分层没有特定的界限。本研究旨在提出ICC的先进节点地位。方法:回顾性分析2000年至2020年在三个三级中心接受肝切除(LR)合并淋巴结清扫(LND)的病理证实的淋巴结阳性ICC患者的资料。评估区域边界和分层总生存(OS)的产量。淋巴结(LN)区域定义如下:肝十二指肠韧带、肝总动脉、胰周区(HCP-area)、胃肝区(GH-area)、主动脉旁区(A-area)。结果:84例淋巴结阳性ICC患者入组本研究。检索到的LNs和涉及的LNs (iln)的中位数分别为15(范围:2-56)和2(范围:1-20)。大多数患者(96.5%)在hcp区域有iln,而只有3例患者(3.5%)在其他未累及hcp区域的区域有iln。局限于hcp区域的LN转移患者的OS优于超出该区域的患者(中位OS: 24.3 vs 13.3个月,p = 0.047)。iln划分OS的最佳临界值为4个,1-3个iln患者的OS优于≥4个iln患者(25.4个月vs 13.8个月,p = 0.006)。与单独使用分布或产量相比,将分布和产量结合使用显示出最好的预后能力。结论:在淋巴结阳性的ICC患者中,淋巴结转移超出hcp区域或≥4个iln可被认为是晚期N疾病。
Defining advanced lymph node metastasis in intrahepatic cholangiocarcinoma: A multicenter study
Background
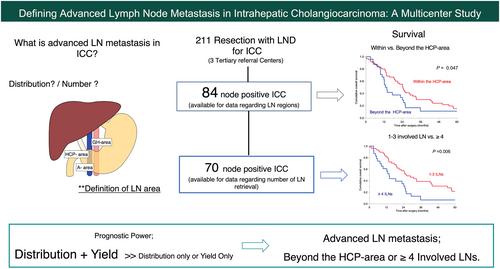
There is no specific boundary for stratifying survival outcomes in patients with node-positive intrahepatic cholangiocarcinoma (ICC). This study aimed to propose advanced nodal status in ICC.
Methods
Data from patients with pathologically confirmed node-positive ICC who underwent liver resection (LR) with lymph node dissection (LND) from 2000 to 2020 at three tertiary centers were retrospectively analyzed. The boundaries of regions and the yield that stratified overall survival (OS) were evaluated. The lymph node (LN) regions were defined as follows: hepatoduodenal ligament, common hepatic artery, and peripancreatic area (HCP-area), gastrohepatic area (GH-area), and para-aortic area (A-area).
Results
Eighty-four patients with node-positive ICC were enrolled in this study. The median numbers of retrieved LNs and involved LNs (ILNs) were 15 (range: 2–56) and 2 (range: 1–20), respectively. Most patients (96.5%) had ILNs in the HCP-area, whereas only 3 patients (3.5%) had ILNs in other areas without HCP-area involvement. OS of patients with LN metastasis confined to the HCP-area was better than for those beyond this area (median OS: 24.3 vs. 13.3 months, p = 0.047). The best cut-off number of ILNs to stratify OS was 4, and patients with 1–3 ILNs showed better OS than those with ≥ 4 ILNs (25.4 vs. 13.8 months, p = 0.006). Combining distribution and yield showed the best prognostic power compared to using either distribution or yield alone.
Conclusion
In patients with node-positive ICC, LN metastasis beyond the HCP-area or ≥ 4 ILNs can be proposed as advanced N disease.
期刊介绍:
Hepatology Research (formerly International Hepatology Communications) is the official journal of the Japan Society of Hepatology, and publishes original articles, reviews and short comunications dealing with hepatology. Reviews or mini-reviews are especially welcomed from those areas within hepatology undergoing rapid changes. Short communications should contain concise definitive information.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


