Yuki Miyazaki, Masato Fujiki, Munkhbold Tuul, Mazhar Khalil, Alejandro Pita, Jaekeun Kim, Andrea Schlegel, Choon H D Kwon, Federico Aucejo, Antonio D Pinna, Charles Miller, Koji Hashimoto
{"title":"受体3-肝静脉技术与移植物静脉成形术在左叶活体肝移植中最大化静脉流出。","authors":"Yuki Miyazaki, Masato Fujiki, Munkhbold Tuul, Mazhar Khalil, Alejandro Pita, Jaekeun Kim, Andrea Schlegel, Choon H D Kwon, Federico Aucejo, Antonio D Pinna, Charles Miller, Koji Hashimoto","doi":"10.1097/TXD.0000000000001778","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Augmentation of hepatic venous outflow is crucial in living donor liver transplantation (LDLT) to maximize functional graft size and prevent venous complications. We present details of our outflow augmentation technique for left lobe grafts (LLG) in adult LDLTs, which uses all recipient 3 hepatic veins and venoplasty of graft left and middle hepatic veins. This study examines the effectiveness of our technique in preventing outflow complications and the correlation between anatomical variations of the graft hepatic veins and surgical outcomes.</p><p><strong>Methods: </strong>We retrospectively reviewed 88 patients who underwent LLG-LDLT between 2012 and 2023. The patients were classified into 3 groups based on the graft hepatic vein anatomy and usage of venoplasty: group 1 (n = 10, common trunk without venoplasty), group 2 (n = 62, common trunk with venoplasty), and group 3 (n = 16, no common trunk with venoplasty).</p><p><strong>Results: </strong>No patient developed clinically significant venous outflow complications or graft loss related to venous outflow. There were no significant differences in complication rates or ascites production among the groups. Five-year graft survival was comparable among the groups (<i>P</i> = 0.43). Multiple regression analysis revealed that the model for end-stage liver disease score was the only independent risk factor for increased ascites after transplant (standardized beta, 0.546; <i>t</i> value,4.20; <i>P</i> < 0.001; 95% confidence interval, 0.287-0.804), but anatomical variations of the graft hepatic veins did not influence ascites output.</p><p><strong>Conclusions: </strong>The recipient 3 hepatic vein outflow augmentation technique with graft venoplasty can be applied to various graft hepatic venous anatomy and effectively prevents outflow-related graft loss in LLG-LDLT.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 5","pages":"e1778"},"PeriodicalIF":1.9000,"publicationDate":"2025-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11984780/pdf/","citationCount":"0","resultStr":"{\"title\":\"Recipient 3-Hepatic Vein Technique with Graft Venoplasty to Maximize Venous Outflow in Left Lobe Living Donor Liver Transplantation.\",\"authors\":\"Yuki Miyazaki, Masato Fujiki, Munkhbold Tuul, Mazhar Khalil, Alejandro Pita, Jaekeun Kim, Andrea Schlegel, Choon H D Kwon, Federico Aucejo, Antonio D Pinna, Charles Miller, Koji Hashimoto\",\"doi\":\"10.1097/TXD.0000000000001778\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Augmentation of hepatic venous outflow is crucial in living donor liver transplantation (LDLT) to maximize functional graft size and prevent venous complications. We present details of our outflow augmentation technique for left lobe grafts (LLG) in adult LDLTs, which uses all recipient 3 hepatic veins and venoplasty of graft left and middle hepatic veins. This study examines the effectiveness of our technique in preventing outflow complications and the correlation between anatomical variations of the graft hepatic veins and surgical outcomes.</p><p><strong>Methods: </strong>We retrospectively reviewed 88 patients who underwent LLG-LDLT between 2012 and 2023. The patients were classified into 3 groups based on the graft hepatic vein anatomy and usage of venoplasty: group 1 (n = 10, common trunk without venoplasty), group 2 (n = 62, common trunk with venoplasty), and group 3 (n = 16, no common trunk with venoplasty).</p><p><strong>Results: </strong>No patient developed clinically significant venous outflow complications or graft loss related to venous outflow. There were no significant differences in complication rates or ascites production among the groups. Five-year graft survival was comparable among the groups (<i>P</i> = 0.43). Multiple regression analysis revealed that the model for end-stage liver disease score was the only independent risk factor for increased ascites after transplant (standardized beta, 0.546; <i>t</i> value,4.20; <i>P</i> < 0.001; 95% confidence interval, 0.287-0.804), but anatomical variations of the graft hepatic veins did not influence ascites output.</p><p><strong>Conclusions: </strong>The recipient 3 hepatic vein outflow augmentation technique with graft venoplasty can be applied to various graft hepatic venous anatomy and effectively prevents outflow-related graft loss in LLG-LDLT.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"11 5\",\"pages\":\"e1778\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-04-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11984780/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001778\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001778","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
Recipient 3-Hepatic Vein Technique with Graft Venoplasty to Maximize Venous Outflow in Left Lobe Living Donor Liver Transplantation.
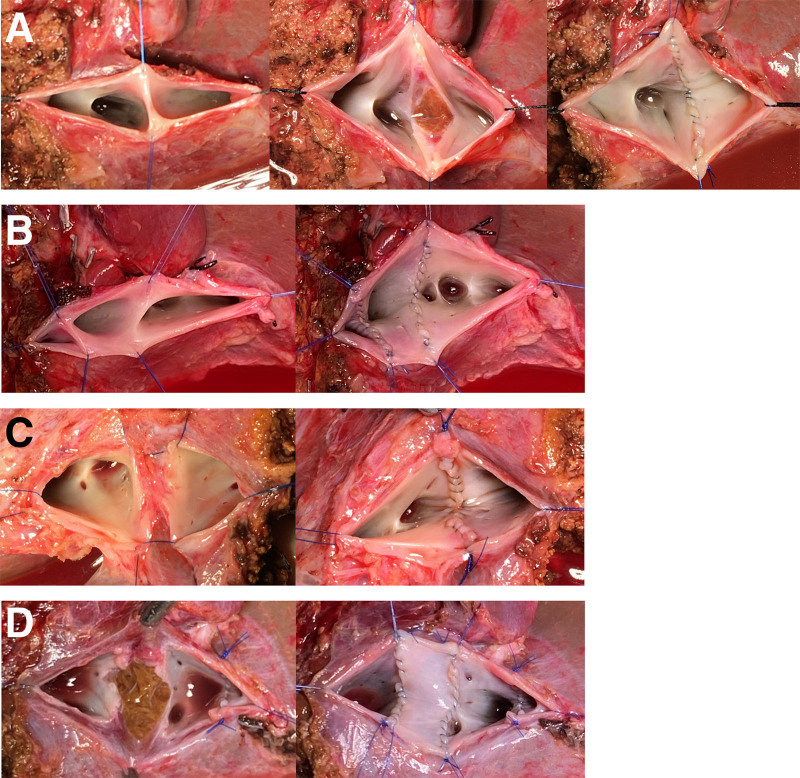
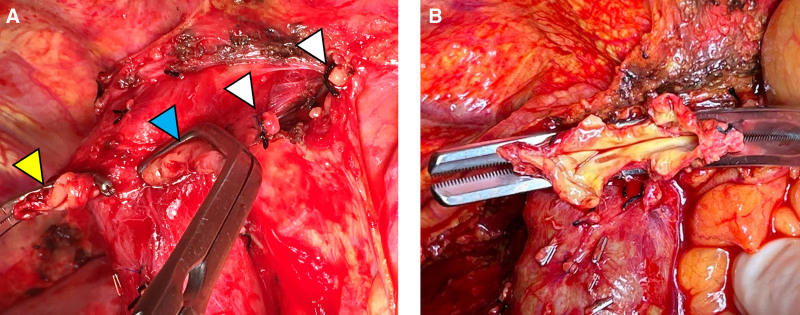
Background: Augmentation of hepatic venous outflow is crucial in living donor liver transplantation (LDLT) to maximize functional graft size and prevent venous complications. We present details of our outflow augmentation technique for left lobe grafts (LLG) in adult LDLTs, which uses all recipient 3 hepatic veins and venoplasty of graft left and middle hepatic veins. This study examines the effectiveness of our technique in preventing outflow complications and the correlation between anatomical variations of the graft hepatic veins and surgical outcomes.
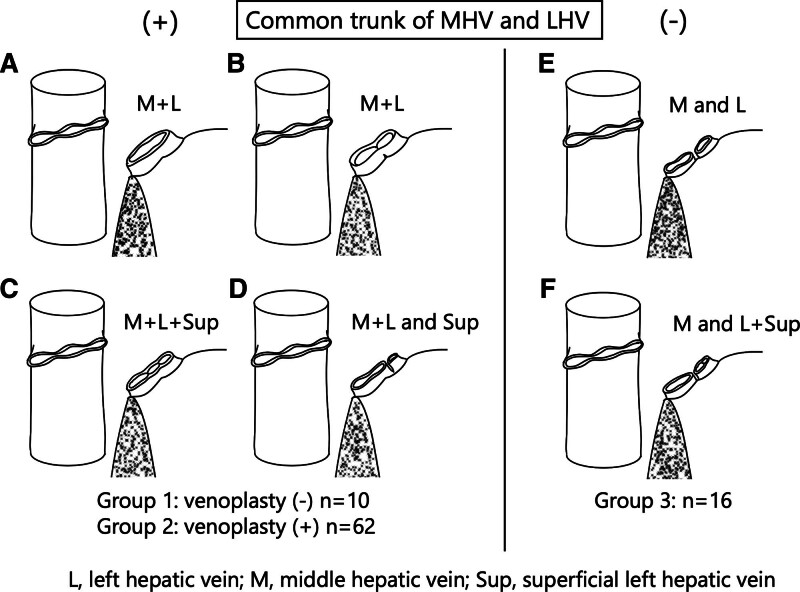
Methods: We retrospectively reviewed 88 patients who underwent LLG-LDLT between 2012 and 2023. The patients were classified into 3 groups based on the graft hepatic vein anatomy and usage of venoplasty: group 1 (n = 10, common trunk without venoplasty), group 2 (n = 62, common trunk with venoplasty), and group 3 (n = 16, no common trunk with venoplasty).
Results: No patient developed clinically significant venous outflow complications or graft loss related to venous outflow. There were no significant differences in complication rates or ascites production among the groups. Five-year graft survival was comparable among the groups (P = 0.43). Multiple regression analysis revealed that the model for end-stage liver disease score was the only independent risk factor for increased ascites after transplant (standardized beta, 0.546; t value,4.20; P < 0.001; 95% confidence interval, 0.287-0.804), but anatomical variations of the graft hepatic veins did not influence ascites output.
Conclusions: The recipient 3 hepatic vein outflow augmentation technique with graft venoplasty can be applied to various graft hepatic venous anatomy and effectively prevents outflow-related graft loss in LLG-LDLT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


