Jordan A Villars, Timothy S Anderson, Jonathan G Yabes, Robert E Schoen, Ravy K Vajravelu
{"title":"质子泵抑制剂使用超过美国食品和药物管理局批准的消化性溃疡患者治疗时间:一项回顾性队列研究","authors":"Jordan A Villars, Timothy S Anderson, Jonathan G Yabes, Robert E Schoen, Ravy K Vajravelu","doi":"10.1002/pds.70152","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Proton-pump inhibitors (PPIs) are effective in treating peptic ulcer disease (PUD), but they are often prescribed beyond the approved duration. Because PPIs are associated with adverse effects, there is a need for effective stewardship.</p><p><strong>Objective: </strong>To identify the frequency of and healthcare factors associated with PPI prescriptions exceeding the approved eight-week treatment duration for PUD.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of patients diagnosed with acute PUD without other indications for PPI use using data from the Veterans Health Administration in the United States. Exposures were patient, provider, and facility factors that could influence PPI prescribing. The outcome was time to a filled PPI prescription exceeding the approved treatment duration for PUD. Associations were assessed using a multivariable time-to-recurrent-event model to calculate adjusted hazard ratios (aHR) and population-attributable fractions. Patients who developed indications for long-term PPI use were censored.</p><p><strong>Results: </strong>We identified 7708 patients with PUD who met eligibility criteria and received PUD treatment (median age 79 [IQR 71-85], 7% female). Thirty-five percent had PPI prescriptions exceeding the approved duration for a median of 346 days (IQR 165-643) of overuse. On the patient level, inpatient PUD diagnosis (aHR 1.32, 95% CI 1.25-1.39), use of nonsteroidal anti-inflammatory drugs (NSAIDs) (aHR 1.26, 95% CI 1.18-1.34), use of anticoagulants (aHR 1.25, 95% CI 1.13-1.38), and moderate frailty (1.15, 95% CI 1.06-1.26) had the strongest associations with filled PPI prescriptions exceeding the approved duration. On the health-system level, inpatient PUD diagnosis had the highest peak population attributable fraction at 0.26, followed by NSAIDs and anticoagulants at 0.18.</p><p><strong>Conclusions: </strong>Markers of patient complexity and medication use not meeting gastroprotection guidelines are associated with inappropriate PPI persistence among patients with PUD. These data may inform future targeted PPI deprescribing programs.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 5","pages":"e70152"},"PeriodicalIF":2.4000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12038380/pdf/","citationCount":"0","resultStr":"{\"title\":\"Proton Pump Inhibitor Use Exceeding the U.S. Food and Drug Administration Approved Treatment Duration for Patients With Peptic Ulcer Disease: A Retrospective Cohort Study.\",\"authors\":\"Jordan A Villars, Timothy S Anderson, Jonathan G Yabes, Robert E Schoen, Ravy K Vajravelu\",\"doi\":\"10.1002/pds.70152\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Proton-pump inhibitors (PPIs) are effective in treating peptic ulcer disease (PUD), but they are often prescribed beyond the approved duration. Because PPIs are associated with adverse effects, there is a need for effective stewardship.</p><p><strong>Objective: </strong>To identify the frequency of and healthcare factors associated with PPI prescriptions exceeding the approved eight-week treatment duration for PUD.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of patients diagnosed with acute PUD without other indications for PPI use using data from the Veterans Health Administration in the United States. Exposures were patient, provider, and facility factors that could influence PPI prescribing. The outcome was time to a filled PPI prescription exceeding the approved treatment duration for PUD. Associations were assessed using a multivariable time-to-recurrent-event model to calculate adjusted hazard ratios (aHR) and population-attributable fractions. Patients who developed indications for long-term PPI use were censored.</p><p><strong>Results: </strong>We identified 7708 patients with PUD who met eligibility criteria and received PUD treatment (median age 79 [IQR 71-85], 7% female). Thirty-five percent had PPI prescriptions exceeding the approved duration for a median of 346 days (IQR 165-643) of overuse. On the patient level, inpatient PUD diagnosis (aHR 1.32, 95% CI 1.25-1.39), use of nonsteroidal anti-inflammatory drugs (NSAIDs) (aHR 1.26, 95% CI 1.18-1.34), use of anticoagulants (aHR 1.25, 95% CI 1.13-1.38), and moderate frailty (1.15, 95% CI 1.06-1.26) had the strongest associations with filled PPI prescriptions exceeding the approved duration. On the health-system level, inpatient PUD diagnosis had the highest peak population attributable fraction at 0.26, followed by NSAIDs and anticoagulants at 0.18.</p><p><strong>Conclusions: </strong>Markers of patient complexity and medication use not meeting gastroprotection guidelines are associated with inappropriate PPI persistence among patients with PUD. These data may inform future targeted PPI deprescribing programs.</p>\",\"PeriodicalId\":19782,\"journal\":{\"name\":\"Pharmacoepidemiology and Drug Safety\",\"volume\":\"34 5\",\"pages\":\"e70152\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12038380/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pharmacoepidemiology and Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/pds.70152\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70152","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
摘要
背景:质子泵抑制剂(PPIs)在治疗消化性溃疡疾病(PUD)方面是有效的,但它们经常超过批准的持续时间。由于质子泵抑制剂与不良反应有关,因此需要有效的管理。目的:确定与PPI处方超过批准的8周治疗期相关的频率和保健因素。方法:我们使用美国退伍军人健康管理局的数据,对诊断为急性PUD且无其他PPI适应症的患者进行了回顾性队列研究。暴露是患者、提供者和设施因素可能影响PPI处方。结果是服用PPI处方的时间超过了批准的PUD治疗时间。使用多变量时间-复发事件模型评估相关性,以计算调整风险比(aHR)和人群归因分数。有长期使用PPI适应症的患者被审查。结果:我们确定了7708例符合资格标准并接受了PUD治疗的PUD患者(中位年龄79岁[IQR 71-85], 7%为女性)。35%的人的PPI处方超过了批准的中位数346天(IQR 165-643)的过量使用时间。在患者水平上,住院患者PUD诊断(aHR 1.32, 95% CI 1.25-1.39)、使用非甾体类抗炎药(NSAIDs) (aHR 1.26, 95% CI 1.18-1.34)、使用抗凝剂(aHR 1.25, 95% CI 1.13-1.38)和中度虚弱(1.15,95% CI 1.06-1.26)与PPI处方超过批准持续时间的相关性最强。在卫生系统层面,住院患者PUD诊断的峰值人群归因分数最高,为0.26,其次是非甾体抗炎药和抗凝血药,为0.18。结论:患者复杂性和不符合胃保护指南的药物使用标记与PUD患者不适当的PPI持续存在相关。这些数据可以为未来有针对性的PPI处方方案提供信息。
Proton Pump Inhibitor Use Exceeding the U.S. Food and Drug Administration Approved Treatment Duration for Patients With Peptic Ulcer Disease: A Retrospective Cohort Study.
Background: Proton-pump inhibitors (PPIs) are effective in treating peptic ulcer disease (PUD), but they are often prescribed beyond the approved duration. Because PPIs are associated with adverse effects, there is a need for effective stewardship.
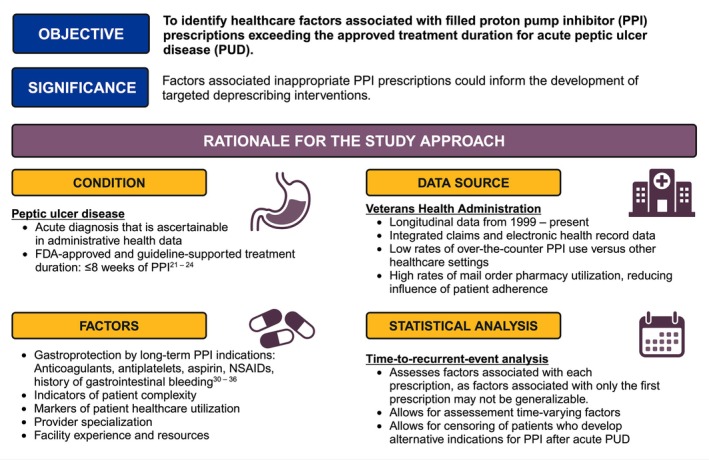
Objective: To identify the frequency of and healthcare factors associated with PPI prescriptions exceeding the approved eight-week treatment duration for PUD.
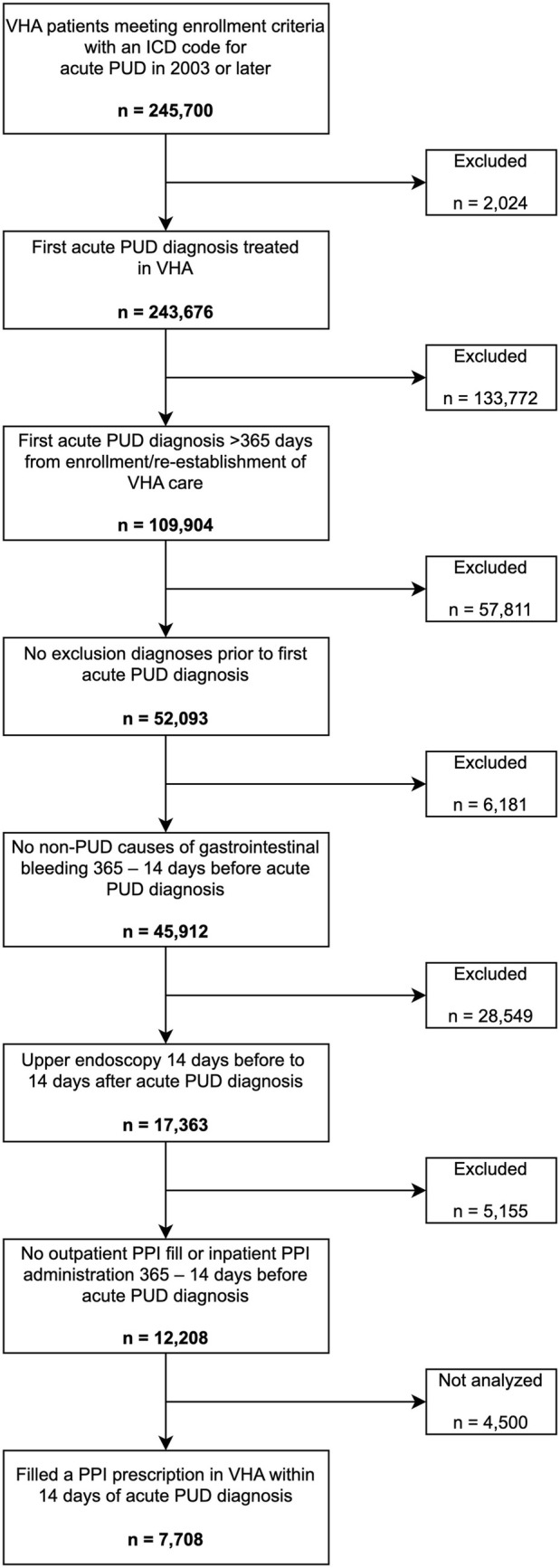
Methods: We conducted a retrospective cohort study of patients diagnosed with acute PUD without other indications for PPI use using data from the Veterans Health Administration in the United States. Exposures were patient, provider, and facility factors that could influence PPI prescribing. The outcome was time to a filled PPI prescription exceeding the approved treatment duration for PUD. Associations were assessed using a multivariable time-to-recurrent-event model to calculate adjusted hazard ratios (aHR) and population-attributable fractions. Patients who developed indications for long-term PPI use were censored.
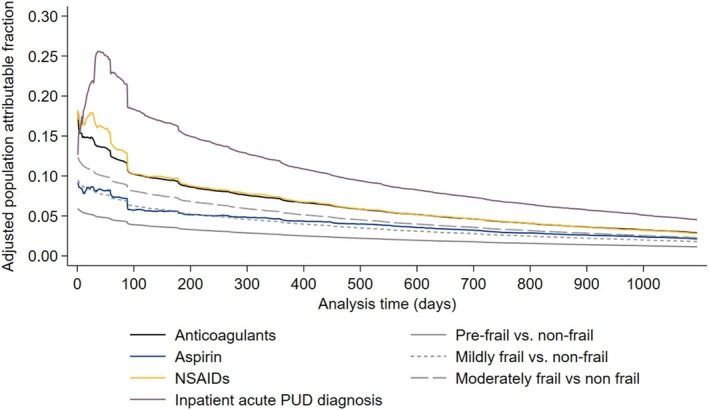
Results: We identified 7708 patients with PUD who met eligibility criteria and received PUD treatment (median age 79 [IQR 71-85], 7% female). Thirty-five percent had PPI prescriptions exceeding the approved duration for a median of 346 days (IQR 165-643) of overuse. On the patient level, inpatient PUD diagnosis (aHR 1.32, 95% CI 1.25-1.39), use of nonsteroidal anti-inflammatory drugs (NSAIDs) (aHR 1.26, 95% CI 1.18-1.34), use of anticoagulants (aHR 1.25, 95% CI 1.13-1.38), and moderate frailty (1.15, 95% CI 1.06-1.26) had the strongest associations with filled PPI prescriptions exceeding the approved duration. On the health-system level, inpatient PUD diagnosis had the highest peak population attributable fraction at 0.26, followed by NSAIDs and anticoagulants at 0.18.
Conclusions: Markers of patient complexity and medication use not meeting gastroprotection guidelines are associated with inappropriate PPI persistence among patients with PUD. These data may inform future targeted PPI deprescribing programs.
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


