Antonella d'Arminio Monforte, Gabriella d'Ettorre, Gioacchino Galardo, Enyal Lani, Eva Kagenaar, Susie Huntington, James Jarrett, Murad Ruf, Walter Ricciardi
{"title":"估计在意大利急诊科引入普遍选择退出艾滋病毒检测的潜在健康经济价值。","authors":"Antonella d'Arminio Monforte, Gabriella d'Ettorre, Gioacchino Galardo, Enyal Lani, Eva Kagenaar, Susie Huntington, James Jarrett, Murad Ruf, Walter Ricciardi","doi":"10.1093/eurpub/ckaf057","DOIUrl":null,"url":null,"abstract":"<p><p>In Italy, an estimated 13 000-15 000 people have undiagnosed HIV, and in 2020, 60% of new diagnoses were late-stage (CD4 < 350 cells/mm3). In hospitals, including emergency departments (EDs), testing is largely limited to indicator-condition-guided testing (IC), with written consent universally required. We developed a closed-cohort hybrid decision tree-Markov model to compare health economic values of two HIV testing strategies in the ED: (1) universal opt-out and (2) IC (Italian standard of care). Data sources included healthcare costs and HIV public health data, obtained from national reports and published studies. A lifetime time horizon and a National Health Service perspective were used. Primary outcomes were life years, quality-adjusted life years (QALYs), and costs. Universal opt-out testing resulted in better health outcomes at higher costs. For every 10 000 individuals attending ED, opt-out testing resulted in 15.78 additional new HIV diagnoses and 14.47 more people linked to HIV care compared with IC. Prevalence threshold analysis demonstrated that opt-out testing was cost-effective compared to IC when the HIV prevalence was 0.25% or higher, assuming a willingness-to-pay threshold of €30 000/QALY. Universal opt-out HIV testing in the ED could be a cost-effective way to increase the number of new HIV diagnoses and improve HIV health outcomes in Italy. The model may underestimate the full benefits of this strategy as our model did not consider disengaged patients or transmissions averted. Further research using real-world data is needed to verify our findings.</p>","PeriodicalId":12059,"journal":{"name":"European Journal of Public Health","volume":" ","pages":"999-1006"},"PeriodicalIF":3.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12529270/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimating the potential health economic value of introducing universal opt-out testing for HIV in emergency departments in Italy.\",\"authors\":\"Antonella d'Arminio Monforte, Gabriella d'Ettorre, Gioacchino Galardo, Enyal Lani, Eva Kagenaar, Susie Huntington, James Jarrett, Murad Ruf, Walter Ricciardi\",\"doi\":\"10.1093/eurpub/ckaf057\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>In Italy, an estimated 13 000-15 000 people have undiagnosed HIV, and in 2020, 60% of new diagnoses were late-stage (CD4 < 350 cells/mm3). In hospitals, including emergency departments (EDs), testing is largely limited to indicator-condition-guided testing (IC), with written consent universally required. We developed a closed-cohort hybrid decision tree-Markov model to compare health economic values of two HIV testing strategies in the ED: (1) universal opt-out and (2) IC (Italian standard of care). Data sources included healthcare costs and HIV public health data, obtained from national reports and published studies. A lifetime time horizon and a National Health Service perspective were used. Primary outcomes were life years, quality-adjusted life years (QALYs), and costs. Universal opt-out testing resulted in better health outcomes at higher costs. For every 10 000 individuals attending ED, opt-out testing resulted in 15.78 additional new HIV diagnoses and 14.47 more people linked to HIV care compared with IC. Prevalence threshold analysis demonstrated that opt-out testing was cost-effective compared to IC when the HIV prevalence was 0.25% or higher, assuming a willingness-to-pay threshold of €30 000/QALY. Universal opt-out HIV testing in the ED could be a cost-effective way to increase the number of new HIV diagnoses and improve HIV health outcomes in Italy. The model may underestimate the full benefits of this strategy as our model did not consider disengaged patients or transmissions averted. Further research using real-world data is needed to verify our findings.</p>\",\"PeriodicalId\":12059,\"journal\":{\"name\":\"European Journal of Public Health\",\"volume\":\" \",\"pages\":\"999-1006\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12529270/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Public Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/eurpub/ckaf057\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Public Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/eurpub/ckaf057","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Estimating the potential health economic value of introducing universal opt-out testing for HIV in emergency departments in Italy.
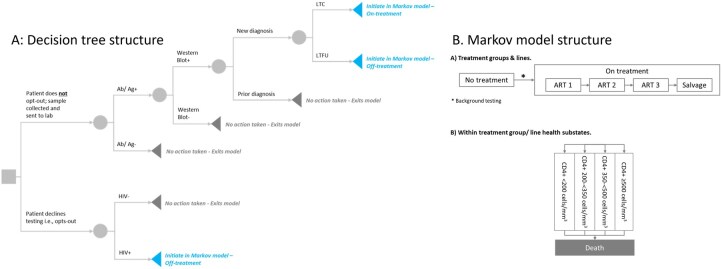
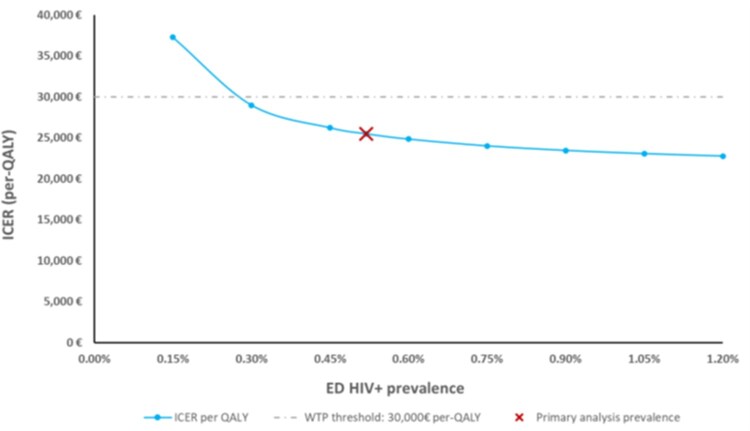
In Italy, an estimated 13 000-15 000 people have undiagnosed HIV, and in 2020, 60% of new diagnoses were late-stage (CD4 < 350 cells/mm3). In hospitals, including emergency departments (EDs), testing is largely limited to indicator-condition-guided testing (IC), with written consent universally required. We developed a closed-cohort hybrid decision tree-Markov model to compare health economic values of two HIV testing strategies in the ED: (1) universal opt-out and (2) IC (Italian standard of care). Data sources included healthcare costs and HIV public health data, obtained from national reports and published studies. A lifetime time horizon and a National Health Service perspective were used. Primary outcomes were life years, quality-adjusted life years (QALYs), and costs. Universal opt-out testing resulted in better health outcomes at higher costs. For every 10 000 individuals attending ED, opt-out testing resulted in 15.78 additional new HIV diagnoses and 14.47 more people linked to HIV care compared with IC. Prevalence threshold analysis demonstrated that opt-out testing was cost-effective compared to IC when the HIV prevalence was 0.25% or higher, assuming a willingness-to-pay threshold of €30 000/QALY. Universal opt-out HIV testing in the ED could be a cost-effective way to increase the number of new HIV diagnoses and improve HIV health outcomes in Italy. The model may underestimate the full benefits of this strategy as our model did not consider disengaged patients or transmissions averted. Further research using real-world data is needed to verify our findings.
期刊介绍:
The European Journal of Public Health (EJPH) is a multidisciplinary journal aimed at attracting contributions from epidemiology, health services research, health economics, social sciences, management sciences, ethics and law, environmental health sciences, and other disciplines of relevance to public health. The journal provides a forum for discussion and debate of current international public health issues, with a focus on the European Region. Bi-monthly issues contain peer-reviewed original articles, editorials, commentaries, book reviews, news, letters to the editor, announcements of events, and various other features.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


