Kyungryong Baek, Joonwon Lee, Kyung-Wan Kim, Seung Hwan Kim, Hyungon Lee, Sung-Chul Jin
{"title":"机械取栓加抢救治疗急性动脉粥样硬化狭窄再通成功后再闭塞的预后因素。","authors":"Kyungryong Baek, Joonwon Lee, Kyung-Wan Kim, Seung Hwan Kim, Hyungon Lee, Sung-Chul Jin","doi":"10.7461/jcen.2025.E2025.02.003","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Treatment failure usually occurs within 24 hours after mechanical thrombectomy (MT) for acute intracranial atherosclerotic steno-occlusion (ICAS) and is an unexpected event that adversely influences the clinical outcome. We retrospectively evaluated the factors influencing reocclusion after MT plus rescue treatment in acute ICAS patients with successful recanalization.</p><p><strong>Methods: </strong>From January 2013 to December 2020, 60 patients with ICAS who underwent MT plus rescue treatment with successful recanalization were included in our study. We classified the patients into a patency group (n=47, 78.3%) and a reocclusion group (n=13, 21.7%) based on CT angiography data obtained the day after MT plus rescue treatment.</p><p><strong>Results: </strong>Intravenous tissue plasminogen activator (IV t-PA) in the patency group (n=18/47 (38.3%)) significantly differed from that in the reocclusion group (n=1/13 (7.7%)) (p=0.045). The number of thrombectomy attempts in the reocclusion group was significantly greater than that in the patency group (median [interquartile range], 2 [1-3] vs. 1 [0-1.5], p=0.004). According to the univariate logistic regression analysis, the only prognostic factor for reocclusion was the number of thrombectomy attempts (odds ratio (OR), 1.655 [1.046-2.619], p=0.032). Conclusions: In our study of ICAS patients who achieved successful recanalization after MT plus rescue treatment, the number of thrombectomy attempts was an independent prognostic factor for reocclusion after MT. Accordingly, for highly suspicious ICAS lesions, additional attempts at the MT should be carefully performed to prevent reocclusion.</p>","PeriodicalId":94072,"journal":{"name":"Journal of cerebrovascular and endovascular neurosurgery","volume":" ","pages":"228-237"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12488330/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic factors for reocclusion after mechanical thrombectomy plus rescue treatment in acute athereosclerotic steno-occlusion with successful recanalization.\",\"authors\":\"Kyungryong Baek, Joonwon Lee, Kyung-Wan Kim, Seung Hwan Kim, Hyungon Lee, Sung-Chul Jin\",\"doi\":\"10.7461/jcen.2025.E2025.02.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Treatment failure usually occurs within 24 hours after mechanical thrombectomy (MT) for acute intracranial atherosclerotic steno-occlusion (ICAS) and is an unexpected event that adversely influences the clinical outcome. We retrospectively evaluated the factors influencing reocclusion after MT plus rescue treatment in acute ICAS patients with successful recanalization.</p><p><strong>Methods: </strong>From January 2013 to December 2020, 60 patients with ICAS who underwent MT plus rescue treatment with successful recanalization were included in our study. We classified the patients into a patency group (n=47, 78.3%) and a reocclusion group (n=13, 21.7%) based on CT angiography data obtained the day after MT plus rescue treatment.</p><p><strong>Results: </strong>Intravenous tissue plasminogen activator (IV t-PA) in the patency group (n=18/47 (38.3%)) significantly differed from that in the reocclusion group (n=1/13 (7.7%)) (p=0.045). The number of thrombectomy attempts in the reocclusion group was significantly greater than that in the patency group (median [interquartile range], 2 [1-3] vs. 1 [0-1.5], p=0.004). According to the univariate logistic regression analysis, the only prognostic factor for reocclusion was the number of thrombectomy attempts (odds ratio (OR), 1.655 [1.046-2.619], p=0.032). Conclusions: In our study of ICAS patients who achieved successful recanalization after MT plus rescue treatment, the number of thrombectomy attempts was an independent prognostic factor for reocclusion after MT. Accordingly, for highly suspicious ICAS lesions, additional attempts at the MT should be carefully performed to prevent reocclusion.</p>\",\"PeriodicalId\":94072,\"journal\":{\"name\":\"Journal of cerebrovascular and endovascular neurosurgery\",\"volume\":\" \",\"pages\":\"228-237\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12488330/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cerebrovascular and endovascular neurosurgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7461/jcen.2025.E2025.02.003\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cerebrovascular and endovascular neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7461/jcen.2025.E2025.02.003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/14 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Prognostic factors for reocclusion after mechanical thrombectomy plus rescue treatment in acute athereosclerotic steno-occlusion with successful recanalization.
Objective: Treatment failure usually occurs within 24 hours after mechanical thrombectomy (MT) for acute intracranial atherosclerotic steno-occlusion (ICAS) and is an unexpected event that adversely influences the clinical outcome. We retrospectively evaluated the factors influencing reocclusion after MT plus rescue treatment in acute ICAS patients with successful recanalization.
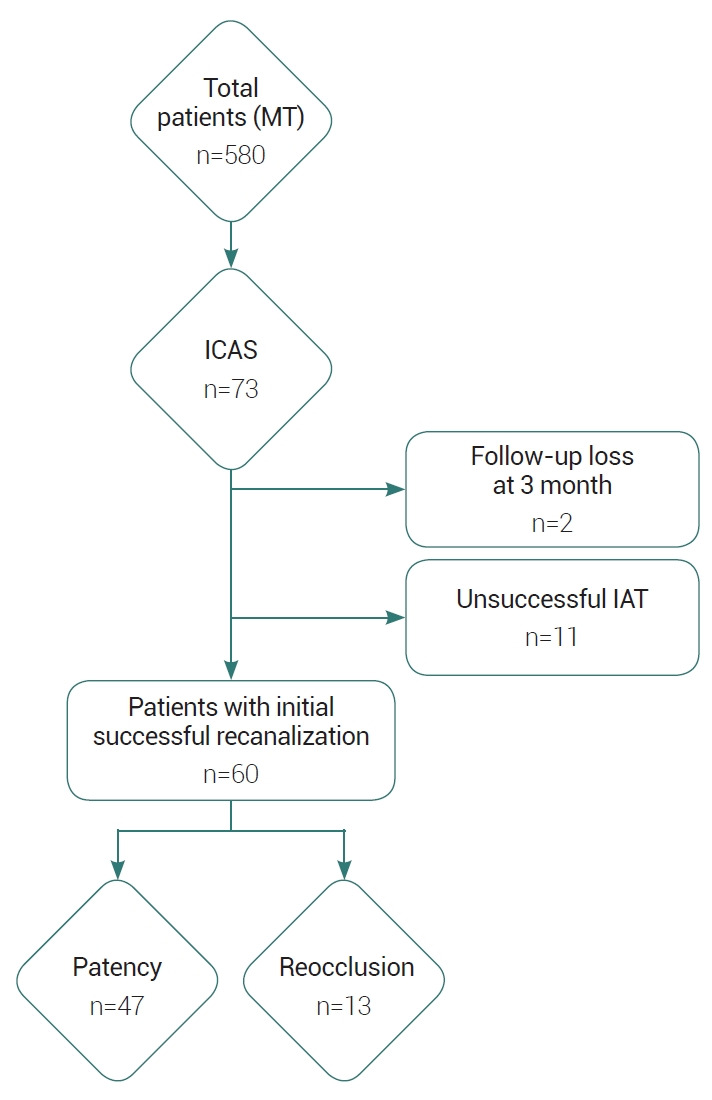
Methods: From January 2013 to December 2020, 60 patients with ICAS who underwent MT plus rescue treatment with successful recanalization were included in our study. We classified the patients into a patency group (n=47, 78.3%) and a reocclusion group (n=13, 21.7%) based on CT angiography data obtained the day after MT plus rescue treatment.
Results: Intravenous tissue plasminogen activator (IV t-PA) in the patency group (n=18/47 (38.3%)) significantly differed from that in the reocclusion group (n=1/13 (7.7%)) (p=0.045). The number of thrombectomy attempts in the reocclusion group was significantly greater than that in the patency group (median [interquartile range], 2 [1-3] vs. 1 [0-1.5], p=0.004). According to the univariate logistic regression analysis, the only prognostic factor for reocclusion was the number of thrombectomy attempts (odds ratio (OR), 1.655 [1.046-2.619], p=0.032). Conclusions: In our study of ICAS patients who achieved successful recanalization after MT plus rescue treatment, the number of thrombectomy attempts was an independent prognostic factor for reocclusion after MT. Accordingly, for highly suspicious ICAS lesions, additional attempts at the MT should be carefully performed to prevent reocclusion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


