James A Swartz, Dana Franceschini, Nora M Marino, Adrienne H Call, Lisa Rosenberger, Sarah Whitehouse
{"title":"在急诊科和其他执业医师中使用丁丙诺啡治疗阿片类药物使用障碍的障碍和促进因素","authors":"James A Swartz, Dana Franceschini, Nora M Marino, Adrienne H Call, Lisa Rosenberger, Sarah Whitehouse","doi":"10.3934/publichealth.2025005","DOIUrl":null,"url":null,"abstract":"<p><p>Despite federal legislation intended to increase the prescribing of buprenorphine as medication for opioid use disorder (MOUD), such as the Drug Addiction Treatment Act (DATA) of 2000, most providers have continued to prescribe to some patients or to not prescribe at all. We aimed to determine the continuing barriers and supports needed for expanding buprenorphine prescribing and compared barriers experienced by emergency department (ED) physicians with those in other practice settings, given the unique aspects of the ED practice setting. We obtained survey data from August through November 2021 from 412 X-waivered Illinois physicians licensed to prescribe buprenorphine as MOUD, 95 (23.1%) of whom worked primarily in a hospital-based ED. Survey questions included: 1) Professional background, practice characteristics, and prescribing practices; 2) barriers to prescribing buprenorphine; 3) barriers to expanding prescribing; and 4) training/additional supports needed to facilitate buprenorphine prescribing. We used bivariate crosstabulations and multivariable OLS and binary logistic regressions to compare the responses of physicians practicing in the ED versus other practice settings and to compare physicians who prescribed buprenorphine in the past year with those who had not. There were few statistically significant differences among the examined subgroups indicating general agreement regardless of practice setting and prescribing status. The most frequently perceived barrier was having an inadequate community-based behavioral health treatment system to which OUD patients could be referred. Insurance reimbursement, difficulties building practice- and community-based systems to support buprenorphine prescribing, and challenges knowing where and how to refer patients for follow-up and ongoing support services were also prominent concerns. Based on study findings, efforts to expand buprenorphine for OUD might focus on providing support to make and manage treatment referrals and expanding the availability of community-based behavioral healthcare services. Building networks of care could potentially have a greater impact on MOUD availability than increasing the number of practitioners trained to prescribe buprenorphine.</p>","PeriodicalId":45684,"journal":{"name":"AIMS Public Health","volume":"12 1","pages":"56-76"},"PeriodicalIF":2.7000,"publicationDate":"2025-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11999815/pdf/","citationCount":"0","resultStr":"{\"title\":\"Barriers and facilitators to prescribing buprenorphine for treating opioid use disorder among emergency department and other practice setting physicians.\",\"authors\":\"James A Swartz, Dana Franceschini, Nora M Marino, Adrienne H Call, Lisa Rosenberger, Sarah Whitehouse\",\"doi\":\"10.3934/publichealth.2025005\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Despite federal legislation intended to increase the prescribing of buprenorphine as medication for opioid use disorder (MOUD), such as the Drug Addiction Treatment Act (DATA) of 2000, most providers have continued to prescribe to some patients or to not prescribe at all. We aimed to determine the continuing barriers and supports needed for expanding buprenorphine prescribing and compared barriers experienced by emergency department (ED) physicians with those in other practice settings, given the unique aspects of the ED practice setting. We obtained survey data from August through November 2021 from 412 X-waivered Illinois physicians licensed to prescribe buprenorphine as MOUD, 95 (23.1%) of whom worked primarily in a hospital-based ED. Survey questions included: 1) Professional background, practice characteristics, and prescribing practices; 2) barriers to prescribing buprenorphine; 3) barriers to expanding prescribing; and 4) training/additional supports needed to facilitate buprenorphine prescribing. We used bivariate crosstabulations and multivariable OLS and binary logistic regressions to compare the responses of physicians practicing in the ED versus other practice settings and to compare physicians who prescribed buprenorphine in the past year with those who had not. There were few statistically significant differences among the examined subgroups indicating general agreement regardless of practice setting and prescribing status. The most frequently perceived barrier was having an inadequate community-based behavioral health treatment system to which OUD patients could be referred. Insurance reimbursement, difficulties building practice- and community-based systems to support buprenorphine prescribing, and challenges knowing where and how to refer patients for follow-up and ongoing support services were also prominent concerns. Based on study findings, efforts to expand buprenorphine for OUD might focus on providing support to make and manage treatment referrals and expanding the availability of community-based behavioral healthcare services. Building networks of care could potentially have a greater impact on MOUD availability than increasing the number of practitioners trained to prescribe buprenorphine.</p>\",\"PeriodicalId\":45684,\"journal\":{\"name\":\"AIMS Public Health\",\"volume\":\"12 1\",\"pages\":\"56-76\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-01-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11999815/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AIMS Public Health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3934/publichealth.2025005\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AIMS Public Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3934/publichealth.2025005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Barriers and facilitators to prescribing buprenorphine for treating opioid use disorder among emergency department and other practice setting physicians.
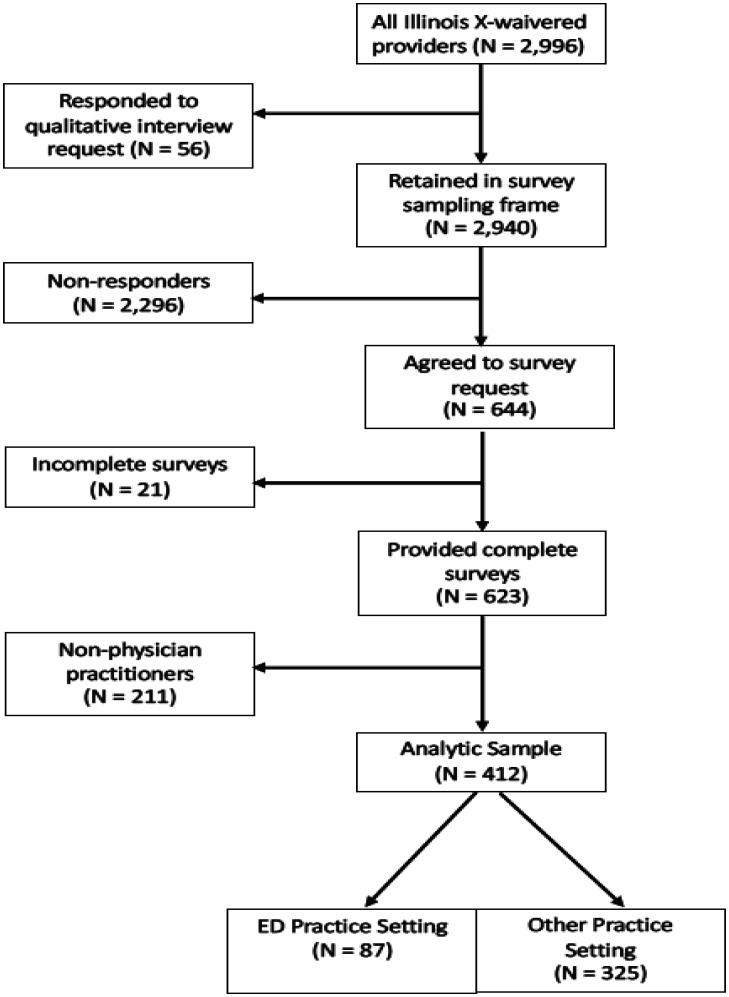
Despite federal legislation intended to increase the prescribing of buprenorphine as medication for opioid use disorder (MOUD), such as the Drug Addiction Treatment Act (DATA) of 2000, most providers have continued to prescribe to some patients or to not prescribe at all. We aimed to determine the continuing barriers and supports needed for expanding buprenorphine prescribing and compared barriers experienced by emergency department (ED) physicians with those in other practice settings, given the unique aspects of the ED practice setting. We obtained survey data from August through November 2021 from 412 X-waivered Illinois physicians licensed to prescribe buprenorphine as MOUD, 95 (23.1%) of whom worked primarily in a hospital-based ED. Survey questions included: 1) Professional background, practice characteristics, and prescribing practices; 2) barriers to prescribing buprenorphine; 3) barriers to expanding prescribing; and 4) training/additional supports needed to facilitate buprenorphine prescribing. We used bivariate crosstabulations and multivariable OLS and binary logistic regressions to compare the responses of physicians practicing in the ED versus other practice settings and to compare physicians who prescribed buprenorphine in the past year with those who had not. There were few statistically significant differences among the examined subgroups indicating general agreement regardless of practice setting and prescribing status. The most frequently perceived barrier was having an inadequate community-based behavioral health treatment system to which OUD patients could be referred. Insurance reimbursement, difficulties building practice- and community-based systems to support buprenorphine prescribing, and challenges knowing where and how to refer patients for follow-up and ongoing support services were also prominent concerns. Based on study findings, efforts to expand buprenorphine for OUD might focus on providing support to make and manage treatment referrals and expanding the availability of community-based behavioral healthcare services. Building networks of care could potentially have a greater impact on MOUD availability than increasing the number of practitioners trained to prescribe buprenorphine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


