Maksim Katsin, Maxim Glebov, Haim Berkenstadt, Dina Orkin, Yotam Portnoy, Adi Shuchami, Amit Yaniv-Rosenfeld, Teddy Lazebnik
{"title":"开发基于机器学习的诱导后低血压预测模型。","authors":"Maksim Katsin, Maxim Glebov, Haim Berkenstadt, Dina Orkin, Yotam Portnoy, Adi Shuchami, Amit Yaniv-Rosenfeld, Teddy Lazebnik","doi":"10.1007/s10877-025-01295-x","DOIUrl":null,"url":null,"abstract":"<p><p>Arterial hypotension is a common and often unintended event during surgery under general anesthesia, associated with increased postoperative complications, such as kidney injury, myocardial injury, and stroke. Postinduction hypotension (PIH) is influenced by patient-specific factors, chronic medication use, and anesthetic induction regimens. Traditional predictive models struggle with this complexity, making machine learning (ML) a promising alternative due to its ability to handle complex datasets and identify hidden patterns. This study aimed to develop and validate an ML-based model for predicting PIH and identifying key clinical predictors. A retrospective cohort study of 20,309 adult patients undergoing non-obstetric surgery under general anesthesia with intravenous induction was conducted. The primary outcome was the occurrence of PIH, defined as mean arterial pressure (MAP) < 55 mmHg within 10 min post-induction. Data were split into training and validation sets using k-fold cross-validation. The model's predictive performance was evaluated using the area under the receiver operating characteristic curve (AUC), and feature importance was assessed using SHapley Additive exPlanations (SHAP) values. PIH occurred in 4,948 patients (24.4%). Key predictors included preinduction systolic and mean arterial pressures, propofol dose, and beta-blocker use. The ML model achieved an AUC of 0.732 in predicting PIH. The ML-based model demonstrated significant predictive capability for PIH, identifying key clinical predictors. This model holds the potential for improving preoperative planning and patient risk stratification. However, further validation through prospective studies is necessary to confirm these findings.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"889-899"},"PeriodicalIF":2.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474600/pdf/","citationCount":"0","resultStr":"{\"title\":\"Developing a machine learning-based prediction model for postinduction hypotension.\",\"authors\":\"Maksim Katsin, Maxim Glebov, Haim Berkenstadt, Dina Orkin, Yotam Portnoy, Adi Shuchami, Amit Yaniv-Rosenfeld, Teddy Lazebnik\",\"doi\":\"10.1007/s10877-025-01295-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Arterial hypotension is a common and often unintended event during surgery under general anesthesia, associated with increased postoperative complications, such as kidney injury, myocardial injury, and stroke. Postinduction hypotension (PIH) is influenced by patient-specific factors, chronic medication use, and anesthetic induction regimens. Traditional predictive models struggle with this complexity, making machine learning (ML) a promising alternative due to its ability to handle complex datasets and identify hidden patterns. This study aimed to develop and validate an ML-based model for predicting PIH and identifying key clinical predictors. A retrospective cohort study of 20,309 adult patients undergoing non-obstetric surgery under general anesthesia with intravenous induction was conducted. The primary outcome was the occurrence of PIH, defined as mean arterial pressure (MAP) < 55 mmHg within 10 min post-induction. Data were split into training and validation sets using k-fold cross-validation. The model's predictive performance was evaluated using the area under the receiver operating characteristic curve (AUC), and feature importance was assessed using SHapley Additive exPlanations (SHAP) values. PIH occurred in 4,948 patients (24.4%). Key predictors included preinduction systolic and mean arterial pressures, propofol dose, and beta-blocker use. The ML model achieved an AUC of 0.732 in predicting PIH. The ML-based model demonstrated significant predictive capability for PIH, identifying key clinical predictors. This model holds the potential for improving preoperative planning and patient risk stratification. However, further validation through prospective studies is necessary to confirm these findings.</p>\",\"PeriodicalId\":15513,\"journal\":{\"name\":\"Journal of Clinical Monitoring and Computing\",\"volume\":\" \",\"pages\":\"889-899\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474600/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Monitoring and Computing\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10877-025-01295-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-025-01295-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/5 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Developing a machine learning-based prediction model for postinduction hypotension.
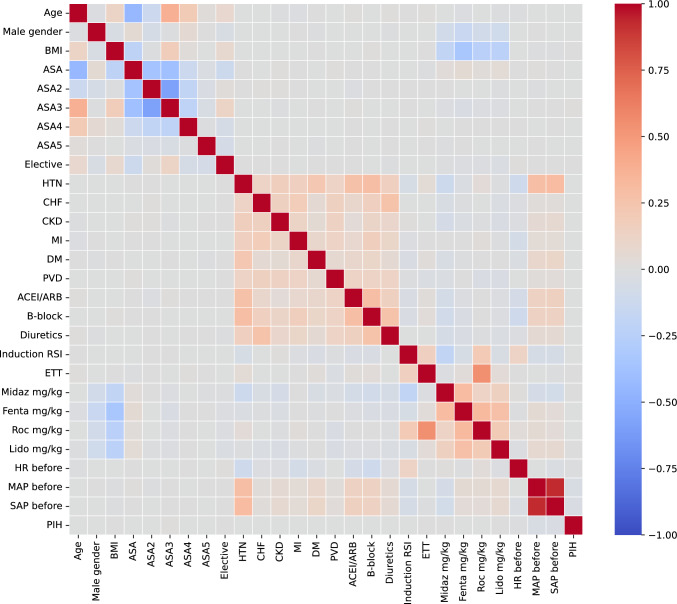
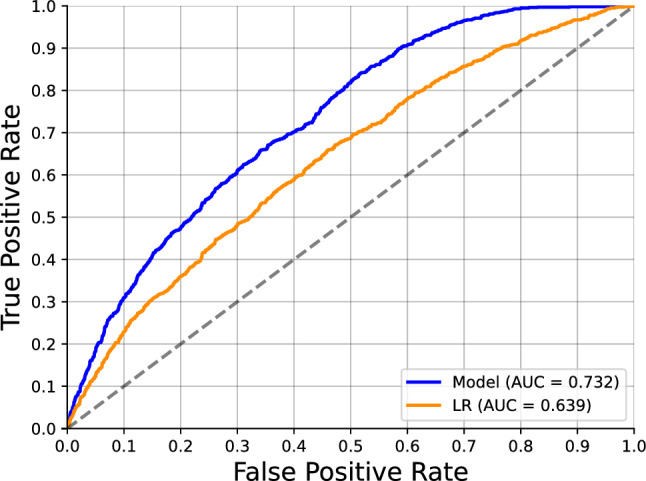
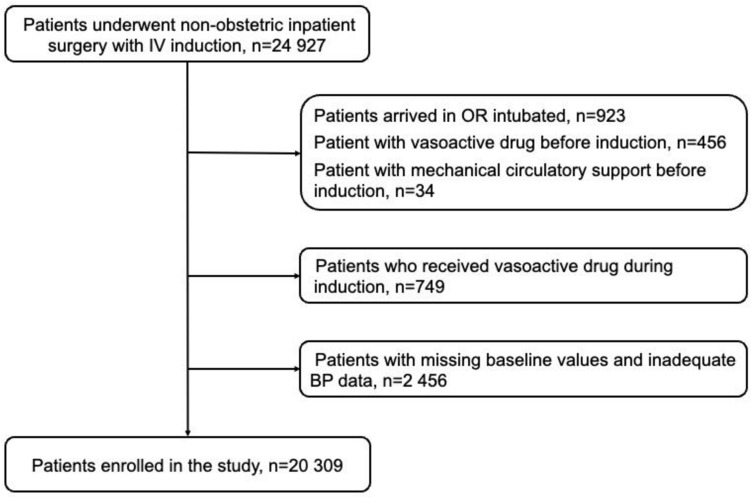
Arterial hypotension is a common and often unintended event during surgery under general anesthesia, associated with increased postoperative complications, such as kidney injury, myocardial injury, and stroke. Postinduction hypotension (PIH) is influenced by patient-specific factors, chronic medication use, and anesthetic induction regimens. Traditional predictive models struggle with this complexity, making machine learning (ML) a promising alternative due to its ability to handle complex datasets and identify hidden patterns. This study aimed to develop and validate an ML-based model for predicting PIH and identifying key clinical predictors. A retrospective cohort study of 20,309 adult patients undergoing non-obstetric surgery under general anesthesia with intravenous induction was conducted. The primary outcome was the occurrence of PIH, defined as mean arterial pressure (MAP) < 55 mmHg within 10 min post-induction. Data were split into training and validation sets using k-fold cross-validation. The model's predictive performance was evaluated using the area under the receiver operating characteristic curve (AUC), and feature importance was assessed using SHapley Additive exPlanations (SHAP) values. PIH occurred in 4,948 patients (24.4%). Key predictors included preinduction systolic and mean arterial pressures, propofol dose, and beta-blocker use. The ML model achieved an AUC of 0.732 in predicting PIH. The ML-based model demonstrated significant predictive capability for PIH, identifying key clinical predictors. This model holds the potential for improving preoperative planning and patient risk stratification. However, further validation through prospective studies is necessary to confirm these findings.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


