Nick Jovanoski, Sarah Vaselenak, Andrew Hogan, Jasmine Turki, Quincy Chu
{"title":"加拿大可切除的alk阳性非小细胞肺癌患者的辅助阿勒替尼与化疗的成本-效果","authors":"Nick Jovanoski, Sarah Vaselenak, Andrew Hogan, Jasmine Turki, Quincy Chu","doi":"10.1007/s40273-025-01488-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>For patients with resected non-small cell lung cancer (NSCLC), the risk of disease recurrence and progression is associated with a substantial humanistic, clinical, and economic burden. In the phase III ALINA trial (NCT03456076), adjuvant alectinib significantly improved disease-free survival (DFS) compared with chemotherapy in patients with resected ALK-positive NSCLC.</p><p><strong>Objective: </strong>The aim of this study was to assess the cost-effectiveness of adjuvant alectinib versus chemotherapy for patients with resected ALK-positive NSCLC in Canada.</p><p><strong>Methods: </strong>A cost-utility model comprising eight health states was developed to estimate lifetime patient outcomes and costs of patients with resected, ALK-positive NSCLC treated with adjuvant alectinib versus platinum-based chemotherapy from a societal perspective. Patterns of disease recurrence and progression were based on ALINA and other trial data; model assumptions were consistent with existing models and validated through consultation with expert Canadian clinicians. Cost-effectiveness was assessed in terms of estimated effect on life-years, quality-adjusted life-years (QALYs), and healthcare costs. In addition, scenario and probabilistic analyses were performed to explore model uncertainty. An annual discount rate of 1.5% was applied to both costs and outcomes (evaluated for 2023).</p><p><strong>Results: </strong>Compared with chemotherapy, alectinib was associated with greater total life-years (19.2 versus 13.1 years) and QALYs (15.0 versus 10.1). Alectinib was dominant over platinum-based chemotherapy as it yielded a lower lifetime cost (CA $480,967.00) versus chemotherapy (CA $592,959.00). Scenario analyses showed model robustness and consistent dominance in cost-effectiveness. Probabilistic analyses results were similar to those from the base case and scenario analyses; alectinib was dominant over chemotherapy in 93.6% of simulations of incremental costs versus incremental QALYs, and remained under a willingness-to-pay threshold of CA$50,000.00 per QALY gained in 99.7% of simulations.</p><p><strong>Conclusions: </strong>Our analysis suggests that adjuvant alectinib is dominant (i.e., more effective and less costly) to platinum-based chemotherapy in Canadian patients with resected ALK-positive NSCLC. Together with the DFS benefit seen in ALINA, this analysis supports adjuvant alectinib as an important new treatment strategy.</p>","PeriodicalId":19807,"journal":{"name":"PharmacoEconomics","volume":" ","pages":"805-817"},"PeriodicalIF":4.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167269/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-Effectiveness of Adjuvant Alectinib Versus Chemotherapy for Patients with Resectable, ALK-positive Non-small Cell Lung Cancer in Canada.\",\"authors\":\"Nick Jovanoski, Sarah Vaselenak, Andrew Hogan, Jasmine Turki, Quincy Chu\",\"doi\":\"10.1007/s40273-025-01488-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>For patients with resected non-small cell lung cancer (NSCLC), the risk of disease recurrence and progression is associated with a substantial humanistic, clinical, and economic burden. In the phase III ALINA trial (NCT03456076), adjuvant alectinib significantly improved disease-free survival (DFS) compared with chemotherapy in patients with resected ALK-positive NSCLC.</p><p><strong>Objective: </strong>The aim of this study was to assess the cost-effectiveness of adjuvant alectinib versus chemotherapy for patients with resected ALK-positive NSCLC in Canada.</p><p><strong>Methods: </strong>A cost-utility model comprising eight health states was developed to estimate lifetime patient outcomes and costs of patients with resected, ALK-positive NSCLC treated with adjuvant alectinib versus platinum-based chemotherapy from a societal perspective. Patterns of disease recurrence and progression were based on ALINA and other trial data; model assumptions were consistent with existing models and validated through consultation with expert Canadian clinicians. Cost-effectiveness was assessed in terms of estimated effect on life-years, quality-adjusted life-years (QALYs), and healthcare costs. In addition, scenario and probabilistic analyses were performed to explore model uncertainty. An annual discount rate of 1.5% was applied to both costs and outcomes (evaluated for 2023).</p><p><strong>Results: </strong>Compared with chemotherapy, alectinib was associated with greater total life-years (19.2 versus 13.1 years) and QALYs (15.0 versus 10.1). Alectinib was dominant over platinum-based chemotherapy as it yielded a lower lifetime cost (CA $480,967.00) versus chemotherapy (CA $592,959.00). Scenario analyses showed model robustness and consistent dominance in cost-effectiveness. Probabilistic analyses results were similar to those from the base case and scenario analyses; alectinib was dominant over chemotherapy in 93.6% of simulations of incremental costs versus incremental QALYs, and remained under a willingness-to-pay threshold of CA$50,000.00 per QALY gained in 99.7% of simulations.</p><p><strong>Conclusions: </strong>Our analysis suggests that adjuvant alectinib is dominant (i.e., more effective and less costly) to platinum-based chemotherapy in Canadian patients with resected ALK-positive NSCLC. Together with the DFS benefit seen in ALINA, this analysis supports adjuvant alectinib as an important new treatment strategy.</p>\",\"PeriodicalId\":19807,\"journal\":{\"name\":\"PharmacoEconomics\",\"volume\":\" \",\"pages\":\"805-817\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167269/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40273-025-01488-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40273-025-01488-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
Cost-Effectiveness of Adjuvant Alectinib Versus Chemotherapy for Patients with Resectable, ALK-positive Non-small Cell Lung Cancer in Canada.
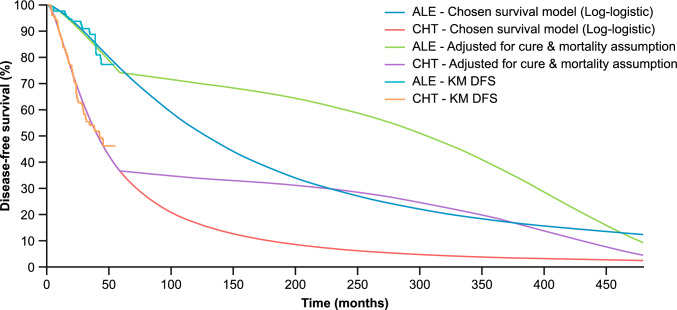
Background: For patients with resected non-small cell lung cancer (NSCLC), the risk of disease recurrence and progression is associated with a substantial humanistic, clinical, and economic burden. In the phase III ALINA trial (NCT03456076), adjuvant alectinib significantly improved disease-free survival (DFS) compared with chemotherapy in patients with resected ALK-positive NSCLC.
Objective: The aim of this study was to assess the cost-effectiveness of adjuvant alectinib versus chemotherapy for patients with resected ALK-positive NSCLC in Canada.
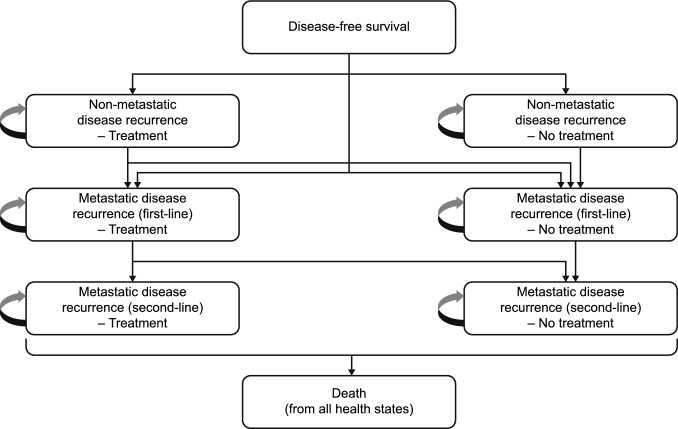
Methods: A cost-utility model comprising eight health states was developed to estimate lifetime patient outcomes and costs of patients with resected, ALK-positive NSCLC treated with adjuvant alectinib versus platinum-based chemotherapy from a societal perspective. Patterns of disease recurrence and progression were based on ALINA and other trial data; model assumptions were consistent with existing models and validated through consultation with expert Canadian clinicians. Cost-effectiveness was assessed in terms of estimated effect on life-years, quality-adjusted life-years (QALYs), and healthcare costs. In addition, scenario and probabilistic analyses were performed to explore model uncertainty. An annual discount rate of 1.5% was applied to both costs and outcomes (evaluated for 2023).
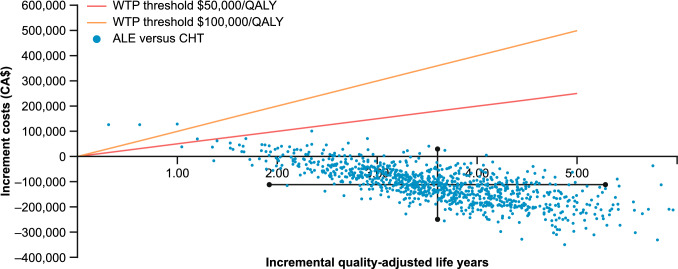
Results: Compared with chemotherapy, alectinib was associated with greater total life-years (19.2 versus 13.1 years) and QALYs (15.0 versus 10.1). Alectinib was dominant over platinum-based chemotherapy as it yielded a lower lifetime cost (CA $480,967.00) versus chemotherapy (CA $592,959.00). Scenario analyses showed model robustness and consistent dominance in cost-effectiveness. Probabilistic analyses results were similar to those from the base case and scenario analyses; alectinib was dominant over chemotherapy in 93.6% of simulations of incremental costs versus incremental QALYs, and remained under a willingness-to-pay threshold of CA$50,000.00 per QALY gained in 99.7% of simulations.
Conclusions: Our analysis suggests that adjuvant alectinib is dominant (i.e., more effective and less costly) to platinum-based chemotherapy in Canadian patients with resected ALK-positive NSCLC. Together with the DFS benefit seen in ALINA, this analysis supports adjuvant alectinib as an important new treatment strategy.
期刊介绍:
PharmacoEconomics is the benchmark journal for peer-reviewed, authoritative and practical articles on the application of pharmacoeconomics and quality-of-life assessment to optimum drug therapy and health outcomes. An invaluable source of applied pharmacoeconomic original research and educational material for the healthcare decision maker.
PharmacoEconomics is dedicated to the clear communication of complex pharmacoeconomic issues related to patient care and drug utilization.
PharmacoEconomics offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by a Key Points summary, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


