George Agathangelou, Matthew Graham-Brown, Aisling C McMahon, George Xydopoulos, Larisa Gofman, Jacob Jaffe
{"title":"英国国民健康服务中人群水平慢性肾脏疾病干预的经济评价","authors":"George Agathangelou, Matthew Graham-Brown, Aisling C McMahon, George Xydopoulos, Larisa Gofman, Jacob Jaffe","doi":"","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Chronic kidney disease (CKD) affects 13% of the global population, is predicted to be the fifth leading cause of premature death by 2040, and is associated with increased risk of cardiovascular disease and acute cardiovascular events. With an aging population and rising diabetes rates, the prevalence of CKD is expected to escalate in the United Kingdom, leading to substantial healthcare costs. When patients reach end-stage kidney disease, interventions such as dialysis and transplantation are required. Dialysis is not only extremely costly but is also associated with a diminished quality of life and significantly elevated mortality. <b>Objectives:</b> This study assesses the cost-effectiveness of several population-level interventions designed to manage CKD, including its progression to end-stage kidney disease. <b>Methods:</b> A population-level Markov model was developed to evaluate the cost-effectiveness and population health impacts of 4 key interventions, individually and combined: (1) early/improved diagnosis, (2) enhanced CKD management, (3) increased use of SGLT-2 inhibitors, and (4) higher rates of pre-emptive live donor transplantation. The model incorporates both NHS direct costs and broader economic impacts, with a 10-year horizon and quarterly cycles. Two scenarios were analyzed: a base case (based on disease progression probabilities) and a constrained case (where growth in the number of patients receiving dialysis and transplantation is limited to historical rates observed in the UK National Health Service). <b>Results:</b> All interventions demonstrated cost-effectiveness, with the combined approach preventing 10 351 deaths and yielding 48 381 quality-adjusted life-years (QALYs) at a cost of £7675 per QALY in the base case scenario. In the constrained scenario, the combined interventions demonstrated cost-effectiveness, preventing 10 026 deaths and yielding 47 514 QALYs at a cost of £22 767 per QALY. <b>Conclusions:</b> The results demonstrate the cost-effectiveness of population level interventions for management of CKD, and the significant burden of dialysis, with avoidance of progression to dialysis a key driver of QALY gains and cost offsets.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 1","pages":"184-190"},"PeriodicalIF":2.3000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12047453/pdf/","citationCount":"0","resultStr":"{\"title\":\"Economic Evaluation of Population-Level Chronic Kidney Disease Interventions in the UK National Health Service.\",\"authors\":\"George Agathangelou, Matthew Graham-Brown, Aisling C McMahon, George Xydopoulos, Larisa Gofman, Jacob Jaffe\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Chronic kidney disease (CKD) affects 13% of the global population, is predicted to be the fifth leading cause of premature death by 2040, and is associated with increased risk of cardiovascular disease and acute cardiovascular events. With an aging population and rising diabetes rates, the prevalence of CKD is expected to escalate in the United Kingdom, leading to substantial healthcare costs. When patients reach end-stage kidney disease, interventions such as dialysis and transplantation are required. Dialysis is not only extremely costly but is also associated with a diminished quality of life and significantly elevated mortality. <b>Objectives:</b> This study assesses the cost-effectiveness of several population-level interventions designed to manage CKD, including its progression to end-stage kidney disease. <b>Methods:</b> A population-level Markov model was developed to evaluate the cost-effectiveness and population health impacts of 4 key interventions, individually and combined: (1) early/improved diagnosis, (2) enhanced CKD management, (3) increased use of SGLT-2 inhibitors, and (4) higher rates of pre-emptive live donor transplantation. The model incorporates both NHS direct costs and broader economic impacts, with a 10-year horizon and quarterly cycles. Two scenarios were analyzed: a base case (based on disease progression probabilities) and a constrained case (where growth in the number of patients receiving dialysis and transplantation is limited to historical rates observed in the UK National Health Service). <b>Results:</b> All interventions demonstrated cost-effectiveness, with the combined approach preventing 10 351 deaths and yielding 48 381 quality-adjusted life-years (QALYs) at a cost of £7675 per QALY in the base case scenario. In the constrained scenario, the combined interventions demonstrated cost-effectiveness, preventing 10 026 deaths and yielding 47 514 QALYs at a cost of £22 767 per QALY. <b>Conclusions:</b> The results demonstrate the cost-effectiveness of population level interventions for management of CKD, and the significant burden of dialysis, with avoidance of progression to dialysis a key driver of QALY gains and cost offsets.</p>\",\"PeriodicalId\":16012,\"journal\":{\"name\":\"Journal of Health Economics and Outcomes Research\",\"volume\":\"12 1\",\"pages\":\"184-190\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12047453/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Health Economics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
Economic Evaluation of Population-Level Chronic Kidney Disease Interventions in the UK National Health Service.
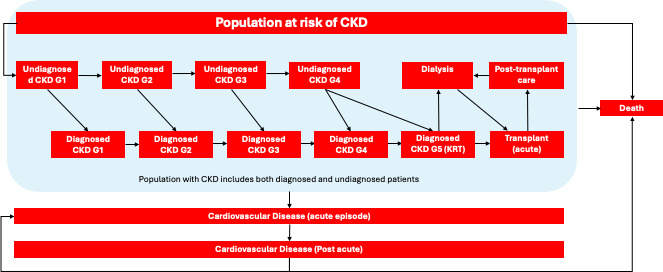
Background: Chronic kidney disease (CKD) affects 13% of the global population, is predicted to be the fifth leading cause of premature death by 2040, and is associated with increased risk of cardiovascular disease and acute cardiovascular events. With an aging population and rising diabetes rates, the prevalence of CKD is expected to escalate in the United Kingdom, leading to substantial healthcare costs. When patients reach end-stage kidney disease, interventions such as dialysis and transplantation are required. Dialysis is not only extremely costly but is also associated with a diminished quality of life and significantly elevated mortality. Objectives: This study assesses the cost-effectiveness of several population-level interventions designed to manage CKD, including its progression to end-stage kidney disease. Methods: A population-level Markov model was developed to evaluate the cost-effectiveness and population health impacts of 4 key interventions, individually and combined: (1) early/improved diagnosis, (2) enhanced CKD management, (3) increased use of SGLT-2 inhibitors, and (4) higher rates of pre-emptive live donor transplantation. The model incorporates both NHS direct costs and broader economic impacts, with a 10-year horizon and quarterly cycles. Two scenarios were analyzed: a base case (based on disease progression probabilities) and a constrained case (where growth in the number of patients receiving dialysis and transplantation is limited to historical rates observed in the UK National Health Service). Results: All interventions demonstrated cost-effectiveness, with the combined approach preventing 10 351 deaths and yielding 48 381 quality-adjusted life-years (QALYs) at a cost of £7675 per QALY in the base case scenario. In the constrained scenario, the combined interventions demonstrated cost-effectiveness, preventing 10 026 deaths and yielding 47 514 QALYs at a cost of £22 767 per QALY. Conclusions: The results demonstrate the cost-effectiveness of population level interventions for management of CKD, and the significant burden of dialysis, with avoidance of progression to dialysis a key driver of QALY gains and cost offsets.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


