Jennifer Le, Julie Huynh, Brandon Vo, Annie Mai, Robert H Mak, Jeremiah D Momper, Edmund V Capparelli, Helen Harvey, Sean Avedissian, Erin Bradley, Amy Sitapati, Karandeep Singh, John S Bradley
{"title":"脓毒症患儿美罗培南分布和清除率的变异性:基于人群的药代动力学与肾脏生物标志物的评估。","authors":"Jennifer Le, Julie Huynh, Brandon Vo, Annie Mai, Robert H Mak, Jeremiah D Momper, Edmund V Capparelli, Helen Harvey, Sean Avedissian, Erin Bradley, Amy Sitapati, Karandeep Singh, John S Bradley","doi":"10.1007/s40262-025-01495-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Meropenem dosing to achieve therapeutic exposure in critically ill children with sepsis is challenging due to a spectrum of renal function, from augmented renal clearance (ARC) to acute kidney injury (AKI). The objective of this study was to define meropenem plasma concentrations and pharmacodynamic exposure metrics in children with septic shock during the first 3 days of PICU hospitalization.</p><p><strong>Methods: </strong>We prospectively evaluated meropenem clearance (CL<sub>MERO</sub>) and volume of distribution (V<sub>1-MERO</sub>), innovatively assessing renal biomarkers (serum creatinine [SCr], serum cystatin C [SCys], and neutrophil gelatinase-associated lipocalin [SNgal]), in infants aged ≥ 4 weeks and children on intravenous (IV) meropenem 20 mg/kg every 8 h from 2019 to 2023. Cases with sepsis were matched to controls without sepsis.</p><p><strong>Results: </strong>Analysis included 27 participants (19 cases and 8 controls) with 309 meropenem serum concentrations. Median age was 11.8 (range 0.6-19.6) years, weight 36.3 (7.2-98.0) kg, SCr 0.33 (0.09-2.57) mg/dL, SCys 451.1 (178.3-1824.1) ng/mL, and SNgal 180.7 (23.2-1403.0) ng/mL. A 2-compartment, population pharmacokinetic (PK) model via NONMEM best described data, with weight on V<sub>MERO</sub> and allometric scaling on CL<sub>MERO</sub>. Using the final model with SCys in V<sub>1-MERO</sub> and estimated glomerular filtration rate (eGFR)-MS in CL<sub>MERO</sub>, the median V<sub>1-MERO</sub> was 0.23 (range 0.07-0.57) L/kg and CL<sub>MERO</sub> 0.15 (0.05-0.49) L/h/kg, with eGFR-MS 139 (23-365) mL/min/1.73 m<sup>2</sup> from AKI to ARC. Meropenem clearance, V<sub>1-MERO</sub> and eGFR-MS were significantly decreased in cases versus controls, with higher variability of eGFR-MS in cases.</p><p><strong>Conclusion: </strong>Wide variation in meropenem concentrations in children with sepsis as compared to those without sepsis prompt close monitoring of GFR and drug concentrations in this population.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":"64 5","pages":"769-777"},"PeriodicalIF":4.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12064575/pdf/","citationCount":"0","resultStr":"{\"title\":\"Variability in Meropenem Distribution and Clearance in Children with Sepsis: Population-Based Pharmacokinetics with Assessment of Renal Biomarkers.\",\"authors\":\"Jennifer Le, Julie Huynh, Brandon Vo, Annie Mai, Robert H Mak, Jeremiah D Momper, Edmund V Capparelli, Helen Harvey, Sean Avedissian, Erin Bradley, Amy Sitapati, Karandeep Singh, John S Bradley\",\"doi\":\"10.1007/s40262-025-01495-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objective: </strong>Meropenem dosing to achieve therapeutic exposure in critically ill children with sepsis is challenging due to a spectrum of renal function, from augmented renal clearance (ARC) to acute kidney injury (AKI). The objective of this study was to define meropenem plasma concentrations and pharmacodynamic exposure metrics in children with septic shock during the first 3 days of PICU hospitalization.</p><p><strong>Methods: </strong>We prospectively evaluated meropenem clearance (CL<sub>MERO</sub>) and volume of distribution (V<sub>1-MERO</sub>), innovatively assessing renal biomarkers (serum creatinine [SCr], serum cystatin C [SCys], and neutrophil gelatinase-associated lipocalin [SNgal]), in infants aged ≥ 4 weeks and children on intravenous (IV) meropenem 20 mg/kg every 8 h from 2019 to 2023. Cases with sepsis were matched to controls without sepsis.</p><p><strong>Results: </strong>Analysis included 27 participants (19 cases and 8 controls) with 309 meropenem serum concentrations. Median age was 11.8 (range 0.6-19.6) years, weight 36.3 (7.2-98.0) kg, SCr 0.33 (0.09-2.57) mg/dL, SCys 451.1 (178.3-1824.1) ng/mL, and SNgal 180.7 (23.2-1403.0) ng/mL. A 2-compartment, population pharmacokinetic (PK) model via NONMEM best described data, with weight on V<sub>MERO</sub> and allometric scaling on CL<sub>MERO</sub>. Using the final model with SCys in V<sub>1-MERO</sub> and estimated glomerular filtration rate (eGFR)-MS in CL<sub>MERO</sub>, the median V<sub>1-MERO</sub> was 0.23 (range 0.07-0.57) L/kg and CL<sub>MERO</sub> 0.15 (0.05-0.49) L/h/kg, with eGFR-MS 139 (23-365) mL/min/1.73 m<sup>2</sup> from AKI to ARC. Meropenem clearance, V<sub>1-MERO</sub> and eGFR-MS were significantly decreased in cases versus controls, with higher variability of eGFR-MS in cases.</p><p><strong>Conclusion: </strong>Wide variation in meropenem concentrations in children with sepsis as compared to those without sepsis prompt close monitoring of GFR and drug concentrations in this population.</p>\",\"PeriodicalId\":10405,\"journal\":{\"name\":\"Clinical Pharmacokinetics\",\"volume\":\"64 5\",\"pages\":\"769-777\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12064575/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacokinetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40262-025-01495-3\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-025-01495-3","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/24 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Variability in Meropenem Distribution and Clearance in Children with Sepsis: Population-Based Pharmacokinetics with Assessment of Renal Biomarkers.
Background and objective: Meropenem dosing to achieve therapeutic exposure in critically ill children with sepsis is challenging due to a spectrum of renal function, from augmented renal clearance (ARC) to acute kidney injury (AKI). The objective of this study was to define meropenem plasma concentrations and pharmacodynamic exposure metrics in children with septic shock during the first 3 days of PICU hospitalization.
Methods: We prospectively evaluated meropenem clearance (CLMERO) and volume of distribution (V1-MERO), innovatively assessing renal biomarkers (serum creatinine [SCr], serum cystatin C [SCys], and neutrophil gelatinase-associated lipocalin [SNgal]), in infants aged ≥ 4 weeks and children on intravenous (IV) meropenem 20 mg/kg every 8 h from 2019 to 2023. Cases with sepsis were matched to controls without sepsis.
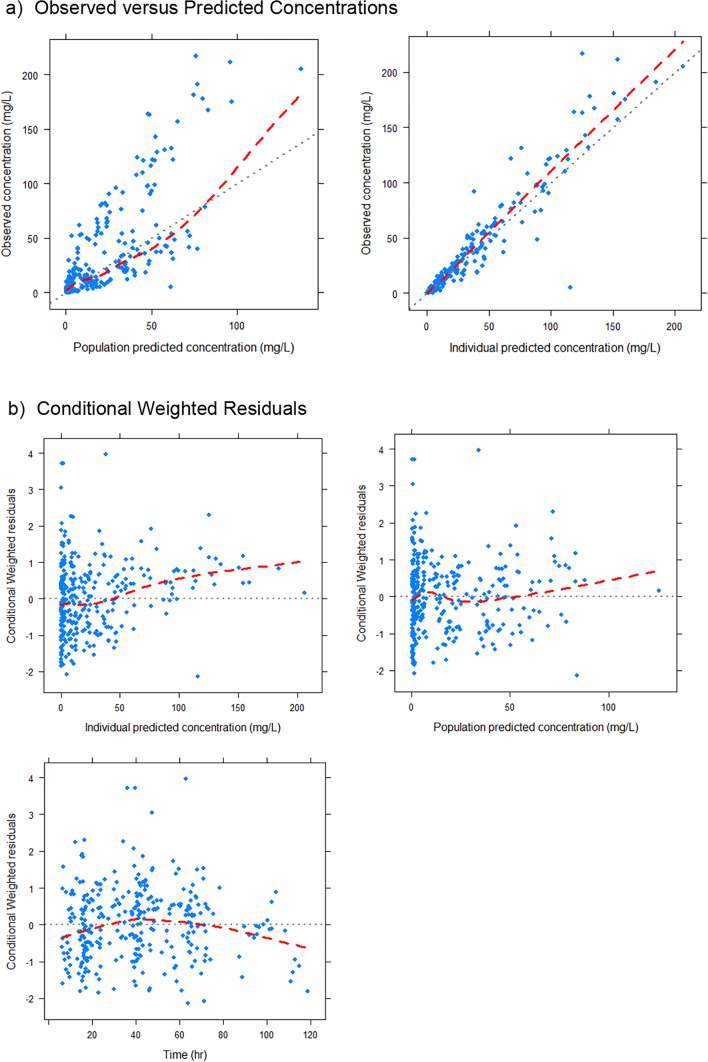
Results: Analysis included 27 participants (19 cases and 8 controls) with 309 meropenem serum concentrations. Median age was 11.8 (range 0.6-19.6) years, weight 36.3 (7.2-98.0) kg, SCr 0.33 (0.09-2.57) mg/dL, SCys 451.1 (178.3-1824.1) ng/mL, and SNgal 180.7 (23.2-1403.0) ng/mL. A 2-compartment, population pharmacokinetic (PK) model via NONMEM best described data, with weight on VMERO and allometric scaling on CLMERO. Using the final model with SCys in V1-MERO and estimated glomerular filtration rate (eGFR)-MS in CLMERO, the median V1-MERO was 0.23 (range 0.07-0.57) L/kg and CLMERO 0.15 (0.05-0.49) L/h/kg, with eGFR-MS 139 (23-365) mL/min/1.73 m2 from AKI to ARC. Meropenem clearance, V1-MERO and eGFR-MS were significantly decreased in cases versus controls, with higher variability of eGFR-MS in cases.
Conclusion: Wide variation in meropenem concentrations in children with sepsis as compared to those without sepsis prompt close monitoring of GFR and drug concentrations in this population.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


