Abigayle Therese R Guiritan, Lee-Boyd D Valencia, Sonia L Chicano
{"title":"阿尔波特综合征在入职前体检中偶然发现蛋白尿:1例报告。","authors":"Abigayle Therese R Guiritan, Lee-Boyd D Valencia, Sonia L Chicano","doi":"10.1155/crin/9933123","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Glomerulonephritis is a prominent cause of chronic kidney disease and encompasses a subset of renal diseases characterized by immune-mediated damage to the basement membrane, the mesangium, or the capillary endothelium. Symptoms in early stages are usually nonspecific and can be easily overlooked. Unfortunately, if not detected early, this may lead to end-stage renal disease. We present a case of a 23-year-old male patient with no family of kidney disease who had proteinuria on routine urinalysis. <b>Case Presentation:</b> A 23-year-old male, nonhypertensive and nondiabetic, with no family history of kidney disease coming in for proteinuria. During pre-employment checkup, patient was noted to have 4+ proteinuria on urinalysis. Creatinine was requested by company doctor with result of 1.05 mg/dL (eGFR: 104 mL/min/1.73 m<sup>2</sup>). Repeat urinalysis was done but still with 4+ proteinuria on urinalysis. Hence, advised consult with a nephrologist due to persistence of proteinuria. Upon consult, workups were done, which revealed hyperuricemia, urate crystals on urinalysis, persistence of 4+ proteinuria, and urine protein creatinine ratio of 2.8 (urine protein: 223.28 mg/dL and urine creatinine: 79.64 mg/dL). Patient was started on ACE inhibitor, hypouricemic agent, and advised kidney biopsy for further evaluation of proteinuria. The review of systems was pertinent for hearing impairment and blurring of vision. Kidney biopsy was done in which electron microscopy showed segmental podocyte foot process effacement. The glomerular basement membrane shows lamellation and alternate thickening and thinning. No definite electron-dense deposits are seen in glomerular basement membrane and mesangium. Mean glomerular basement membrane thickness is 299 nm (normal mean glomerular basement membrane thickness in adult males is 373 ± 42 nm). He was advised consult with an ophthalmologist and otolaryngologist. Regular checkup, monitoring of renal parameters, and appropriate medications were given. <b>Conclusion:</b> Although a rare cause of glomerulonephritis, Alport syndrome must be considered in patients presenting with subnephrotic range proteinuria and microscopic hematuria. Thorough history and physical examination and characteristic findings on kidney biopsy can help in the prompt diagnosis of the disease. Multidisciplinary care and early intervention can improve the quality of life and delay the progression to end-stage kidney disease among these patients.</p>","PeriodicalId":9604,"journal":{"name":"Case Reports in Nephrology","volume":"2025 ","pages":"9933123"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11985237/pdf/","citationCount":"0","resultStr":"{\"title\":\"Alport Syndrome Presenting as Incidental Finding of Proteinuria on Pre-Employment Checkup: A Case Report.\",\"authors\":\"Abigayle Therese R Guiritan, Lee-Boyd D Valencia, Sonia L Chicano\",\"doi\":\"10.1155/crin/9933123\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction:</b> Glomerulonephritis is a prominent cause of chronic kidney disease and encompasses a subset of renal diseases characterized by immune-mediated damage to the basement membrane, the mesangium, or the capillary endothelium. Symptoms in early stages are usually nonspecific and can be easily overlooked. Unfortunately, if not detected early, this may lead to end-stage renal disease. We present a case of a 23-year-old male patient with no family of kidney disease who had proteinuria on routine urinalysis. <b>Case Presentation:</b> A 23-year-old male, nonhypertensive and nondiabetic, with no family history of kidney disease coming in for proteinuria. During pre-employment checkup, patient was noted to have 4+ proteinuria on urinalysis. Creatinine was requested by company doctor with result of 1.05 mg/dL (eGFR: 104 mL/min/1.73 m<sup>2</sup>). Repeat urinalysis was done but still with 4+ proteinuria on urinalysis. Hence, advised consult with a nephrologist due to persistence of proteinuria. Upon consult, workups were done, which revealed hyperuricemia, urate crystals on urinalysis, persistence of 4+ proteinuria, and urine protein creatinine ratio of 2.8 (urine protein: 223.28 mg/dL and urine creatinine: 79.64 mg/dL). Patient was started on ACE inhibitor, hypouricemic agent, and advised kidney biopsy for further evaluation of proteinuria. The review of systems was pertinent for hearing impairment and blurring of vision. Kidney biopsy was done in which electron microscopy showed segmental podocyte foot process effacement. The glomerular basement membrane shows lamellation and alternate thickening and thinning. No definite electron-dense deposits are seen in glomerular basement membrane and mesangium. Mean glomerular basement membrane thickness is 299 nm (normal mean glomerular basement membrane thickness in adult males is 373 ± 42 nm). He was advised consult with an ophthalmologist and otolaryngologist. Regular checkup, monitoring of renal parameters, and appropriate medications were given. <b>Conclusion:</b> Although a rare cause of glomerulonephritis, Alport syndrome must be considered in patients presenting with subnephrotic range proteinuria and microscopic hematuria. Thorough history and physical examination and characteristic findings on kidney biopsy can help in the prompt diagnosis of the disease. Multidisciplinary care and early intervention can improve the quality of life and delay the progression to end-stage kidney disease among these patients.</p>\",\"PeriodicalId\":9604,\"journal\":{\"name\":\"Case Reports in Nephrology\",\"volume\":\"2025 \",\"pages\":\"9933123\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-02-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11985237/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crin/9933123\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crin/9933123","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Alport Syndrome Presenting as Incidental Finding of Proteinuria on Pre-Employment Checkup: A Case Report.
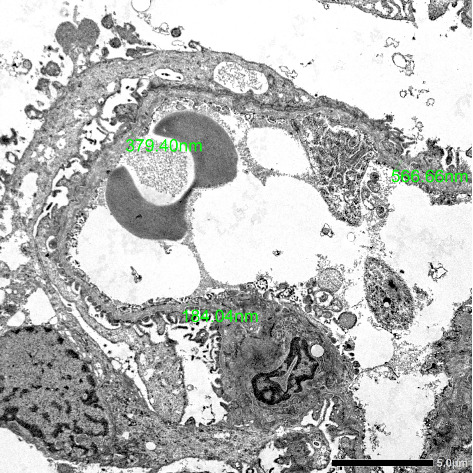
Introduction: Glomerulonephritis is a prominent cause of chronic kidney disease and encompasses a subset of renal diseases characterized by immune-mediated damage to the basement membrane, the mesangium, or the capillary endothelium. Symptoms in early stages are usually nonspecific and can be easily overlooked. Unfortunately, if not detected early, this may lead to end-stage renal disease. We present a case of a 23-year-old male patient with no family of kidney disease who had proteinuria on routine urinalysis. Case Presentation: A 23-year-old male, nonhypertensive and nondiabetic, with no family history of kidney disease coming in for proteinuria. During pre-employment checkup, patient was noted to have 4+ proteinuria on urinalysis. Creatinine was requested by company doctor with result of 1.05 mg/dL (eGFR: 104 mL/min/1.73 m2). Repeat urinalysis was done but still with 4+ proteinuria on urinalysis. Hence, advised consult with a nephrologist due to persistence of proteinuria. Upon consult, workups were done, which revealed hyperuricemia, urate crystals on urinalysis, persistence of 4+ proteinuria, and urine protein creatinine ratio of 2.8 (urine protein: 223.28 mg/dL and urine creatinine: 79.64 mg/dL). Patient was started on ACE inhibitor, hypouricemic agent, and advised kidney biopsy for further evaluation of proteinuria. The review of systems was pertinent for hearing impairment and blurring of vision. Kidney biopsy was done in which electron microscopy showed segmental podocyte foot process effacement. The glomerular basement membrane shows lamellation and alternate thickening and thinning. No definite electron-dense deposits are seen in glomerular basement membrane and mesangium. Mean glomerular basement membrane thickness is 299 nm (normal mean glomerular basement membrane thickness in adult males is 373 ± 42 nm). He was advised consult with an ophthalmologist and otolaryngologist. Regular checkup, monitoring of renal parameters, and appropriate medications were given. Conclusion: Although a rare cause of glomerulonephritis, Alport syndrome must be considered in patients presenting with subnephrotic range proteinuria and microscopic hematuria. Thorough history and physical examination and characteristic findings on kidney biopsy can help in the prompt diagnosis of the disease. Multidisciplinary care and early intervention can improve the quality of life and delay the progression to end-stage kidney disease among these patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


