Christoph P Hornik, Henry P Foote, Eric Kendig, John Mohr
{"title":"一个成人人群药代动力学模型来模拟在患有心力衰竭和容量负荷的青少年中皮下给药固定剂量速尿。","authors":"Christoph P Hornik, Henry P Foote, Eric Kendig, John Mohr","doi":"10.1007/s40262-025-01515-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Subcutaneous furosemide administered with the On-Body Infusor could be useful in children with heart failure (HF) and congestion due to volume overload, but the appropriate dosing regimen is unknown.</p><p><strong>Objective: </strong>This study aimed to develop a population pharmacokinetic (popPK) model to determine the subcutaneous furosemide dosing regimen in children with HF who are appropriate for On-Body Infusor use.</p><p><strong>Methods: </strong>Samples collected from 15 adults with HF who received subcutaneous or intravenous furosemide in a randomized phase II/III study (NCT02329834) were used to develop the popPK model with covariates identified by forward inclusion and backward elimination; validation was by bootstrapping. The model was allometrically scaled from a 70-kg adult body weight to simulate furosemide pharmacokinetics in virtual adolescents aged 12-17 years by weight category (42.5-50.0, > 50-60, and > 60-70 kg) for subcutaneous furosemide 80 mg (30 mg over 1 h then 12.5 mg/h for 4 h).</p><p><strong>Results: </strong>Furosemide pharmacokinetics were best characterized using a two-compartment model with first-order absorption and elimination. After scaling to adolescents in subcutaneous dosing simulations, estimated furosemide clearance was 1.55 mL/min/kg. Estimated exposure (mean area under the plasma concentration-time curve at 24 h) was 16,800 µg⋅h/L in adolescents weighing 42.5-50.0 kg, 14,700 µg⋅h/L in adolescents weighing > 50-60 kg, and 13,000 µg⋅h/L in adolescents weighing > 60-70 kg versus 12,400 µg⋅h/L in adults.</p><p><strong>Conclusions: </strong>Simulated furosemide exposure was consistent with published values, supporting an 80-mg dose of subcutaneous furosemide (30 mg over the first hour, then 12.5 mg/h for 4 h) for adolescents aged 12-17 years with body weight ≥ 42.5 kg.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"899-908"},"PeriodicalIF":4.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12159125/pdf/","citationCount":"0","resultStr":"{\"title\":\"An Adult Population Pharmacokinetic Model to Simulate Subcutaneous Administration of a Fixed Dose of Furosemide in Adolescents with Heart Failure and Volume Overload.\",\"authors\":\"Christoph P Hornik, Henry P Foote, Eric Kendig, John Mohr\",\"doi\":\"10.1007/s40262-025-01515-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Subcutaneous furosemide administered with the On-Body Infusor could be useful in children with heart failure (HF) and congestion due to volume overload, but the appropriate dosing regimen is unknown.</p><p><strong>Objective: </strong>This study aimed to develop a population pharmacokinetic (popPK) model to determine the subcutaneous furosemide dosing regimen in children with HF who are appropriate for On-Body Infusor use.</p><p><strong>Methods: </strong>Samples collected from 15 adults with HF who received subcutaneous or intravenous furosemide in a randomized phase II/III study (NCT02329834) were used to develop the popPK model with covariates identified by forward inclusion and backward elimination; validation was by bootstrapping. The model was allometrically scaled from a 70-kg adult body weight to simulate furosemide pharmacokinetics in virtual adolescents aged 12-17 years by weight category (42.5-50.0, > 50-60, and > 60-70 kg) for subcutaneous furosemide 80 mg (30 mg over 1 h then 12.5 mg/h for 4 h).</p><p><strong>Results: </strong>Furosemide pharmacokinetics were best characterized using a two-compartment model with first-order absorption and elimination. After scaling to adolescents in subcutaneous dosing simulations, estimated furosemide clearance was 1.55 mL/min/kg. Estimated exposure (mean area under the plasma concentration-time curve at 24 h) was 16,800 µg⋅h/L in adolescents weighing 42.5-50.0 kg, 14,700 µg⋅h/L in adolescents weighing > 50-60 kg, and 13,000 µg⋅h/L in adolescents weighing > 60-70 kg versus 12,400 µg⋅h/L in adults.</p><p><strong>Conclusions: </strong>Simulated furosemide exposure was consistent with published values, supporting an 80-mg dose of subcutaneous furosemide (30 mg over the first hour, then 12.5 mg/h for 4 h) for adolescents aged 12-17 years with body weight ≥ 42.5 kg.</p>\",\"PeriodicalId\":10405,\"journal\":{\"name\":\"Clinical Pharmacokinetics\",\"volume\":\" \",\"pages\":\"899-908\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12159125/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacokinetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40262-025-01515-2\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-025-01515-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/13 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
An Adult Population Pharmacokinetic Model to Simulate Subcutaneous Administration of a Fixed Dose of Furosemide in Adolescents with Heart Failure and Volume Overload.
Background: Subcutaneous furosemide administered with the On-Body Infusor could be useful in children with heart failure (HF) and congestion due to volume overload, but the appropriate dosing regimen is unknown.
Objective: This study aimed to develop a population pharmacokinetic (popPK) model to determine the subcutaneous furosemide dosing regimen in children with HF who are appropriate for On-Body Infusor use.
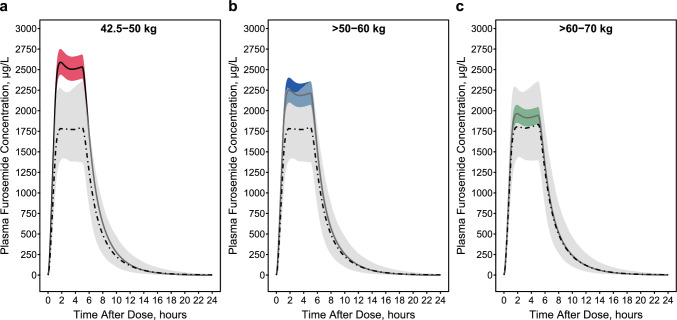
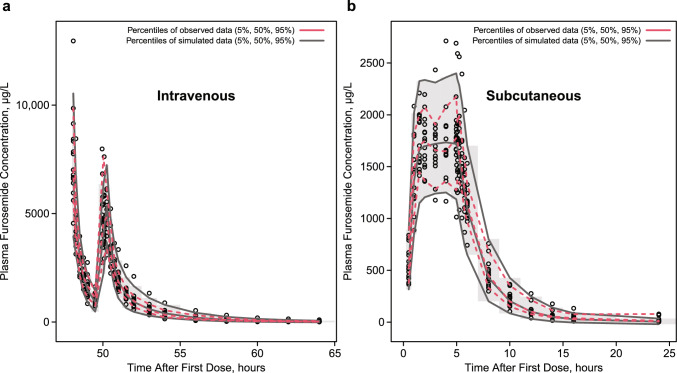
Methods: Samples collected from 15 adults with HF who received subcutaneous or intravenous furosemide in a randomized phase II/III study (NCT02329834) were used to develop the popPK model with covariates identified by forward inclusion and backward elimination; validation was by bootstrapping. The model was allometrically scaled from a 70-kg adult body weight to simulate furosemide pharmacokinetics in virtual adolescents aged 12-17 years by weight category (42.5-50.0, > 50-60, and > 60-70 kg) for subcutaneous furosemide 80 mg (30 mg over 1 h then 12.5 mg/h for 4 h).
Results: Furosemide pharmacokinetics were best characterized using a two-compartment model with first-order absorption and elimination. After scaling to adolescents in subcutaneous dosing simulations, estimated furosemide clearance was 1.55 mL/min/kg. Estimated exposure (mean area under the plasma concentration-time curve at 24 h) was 16,800 µg⋅h/L in adolescents weighing 42.5-50.0 kg, 14,700 µg⋅h/L in adolescents weighing > 50-60 kg, and 13,000 µg⋅h/L in adolescents weighing > 60-70 kg versus 12,400 µg⋅h/L in adults.
Conclusions: Simulated furosemide exposure was consistent with published values, supporting an 80-mg dose of subcutaneous furosemide (30 mg over the first hour, then 12.5 mg/h for 4 h) for adolescents aged 12-17 years with body weight ≥ 42.5 kg.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


