David Rozenblat, Arnaud Serret-Larmande, Alexis Maillard, Romain Arrestier, Sarah Benghanem, Julien Charpentier, Michael Darmon, Vincent Das, François Dépret, Jean Luc Donay, Hervé Jacquier, Hélène Poupet, Jean-Michel Molina, Matthieu Lafaurie
{"title":"氨基糖苷类药物对尿脓毒症患者存活率和肾脏预后的影响:一项多中心回顾性研究。","authors":"David Rozenblat, Arnaud Serret-Larmande, Alexis Maillard, Romain Arrestier, Sarah Benghanem, Julien Charpentier, Michael Darmon, Vincent Das, François Dépret, Jean Luc Donay, Hervé Jacquier, Hélène Poupet, Jean-Michel Molina, Matthieu Lafaurie","doi":"10.1186/s13613-025-01469-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Combination therapy with a beta-lactam and an aminoglycoside is currently recommended for the empirical treatment of urosepsis. Nephrotoxicity is the most common adverse effect of aminoglycosides and acute kidney injury (AKI) has a significant prognostic impact in septic shock. This study aimed to evaluate the impact of empirical antibiotic therapy with or without an aminoglycoside on survival and renal outcomes in patients admitted to the intensive care unit (ICU) with urosepsis.</p><p><strong>Methods: </strong>This multicenter, retrospective, comparative study included all adults admitted to the ICU for urinary sepsis or septic shock between January 2015 and May 2022 in four ICUs of three university hospitals within the Assistance Publique-Hôpitaux de Paris (APHP). The primary outcome was mortality on day 30 after ICU admission. Secondary endpoints included the lack of renal recovery, the need for new renal replacement therapy (RRT), the Major Adverse Kidney Events at day 30 (MAKE 30) and ICU length of stay. Confounding by indication was taken into account using propensity score weighting.</p><p><strong>Results: </strong>A total of 580 patients were included, median age was 69 years (interquartile: 58-77) and 53.6% were male. Overall, 335 patients (57.8%) were in septic shock and 448 (79.2%) had AKI on admission. A total of 579 patients (99.8%) received a beta-lactam as empirical therapy (with (n = 444) or without (n = 136) aminoglycosides). The overall 30-day mortality rate was 10.5% (61/580). After propensity score weighting, the mortality rate in patients receiving aminoglycosides was 7.7% (7/91) compared to 12.1% (11/91) in those not receiving aminoglycosides (adjusted hazard ratio (aHR) = 0.65 [0.35; 1.23], p = 0.19). No significant differences were found in the lack of renal recovery at day 30 (aHR = 0.88 [0.49; 1.58], p = 0.67), the need for new RRT within 30 days (aHR = 1.01 [0.54; 1.88], p = 0.97), MAKE 30 (aHR = 0.94 [0.60; 1.50], p = 0.81), and ICU length of stay among survivors (aHR = 1.07 [0.87; 1.31], p = 0.53).</p><p><strong>Conclusions: </strong>Including aminoglycosides in the empirical antibiotic therapy did not significantly improve 30-day survival in patients admitted to the ICU for urosepsis. However, the use of aminoglycosides was not associated with worse renal outcomes.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"52"},"PeriodicalIF":5.5000,"publicationDate":"2025-04-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11992283/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of aminoglycosides on survival rate and renal outcomes in patients with urosepsis: a multicenter retrospective study.\",\"authors\":\"David Rozenblat, Arnaud Serret-Larmande, Alexis Maillard, Romain Arrestier, Sarah Benghanem, Julien Charpentier, Michael Darmon, Vincent Das, François Dépret, Jean Luc Donay, Hervé Jacquier, Hélène Poupet, Jean-Michel Molina, Matthieu Lafaurie\",\"doi\":\"10.1186/s13613-025-01469-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Combination therapy with a beta-lactam and an aminoglycoside is currently recommended for the empirical treatment of urosepsis. Nephrotoxicity is the most common adverse effect of aminoglycosides and acute kidney injury (AKI) has a significant prognostic impact in septic shock. This study aimed to evaluate the impact of empirical antibiotic therapy with or without an aminoglycoside on survival and renal outcomes in patients admitted to the intensive care unit (ICU) with urosepsis.</p><p><strong>Methods: </strong>This multicenter, retrospective, comparative study included all adults admitted to the ICU for urinary sepsis or septic shock between January 2015 and May 2022 in four ICUs of three university hospitals within the Assistance Publique-Hôpitaux de Paris (APHP). The primary outcome was mortality on day 30 after ICU admission. Secondary endpoints included the lack of renal recovery, the need for new renal replacement therapy (RRT), the Major Adverse Kidney Events at day 30 (MAKE 30) and ICU length of stay. Confounding by indication was taken into account using propensity score weighting.</p><p><strong>Results: </strong>A total of 580 patients were included, median age was 69 years (interquartile: 58-77) and 53.6% were male. Overall, 335 patients (57.8%) were in septic shock and 448 (79.2%) had AKI on admission. A total of 579 patients (99.8%) received a beta-lactam as empirical therapy (with (n = 444) or without (n = 136) aminoglycosides). The overall 30-day mortality rate was 10.5% (61/580). After propensity score weighting, the mortality rate in patients receiving aminoglycosides was 7.7% (7/91) compared to 12.1% (11/91) in those not receiving aminoglycosides (adjusted hazard ratio (aHR) = 0.65 [0.35; 1.23], p = 0.19). No significant differences were found in the lack of renal recovery at day 30 (aHR = 0.88 [0.49; 1.58], p = 0.67), the need for new RRT within 30 days (aHR = 1.01 [0.54; 1.88], p = 0.97), MAKE 30 (aHR = 0.94 [0.60; 1.50], p = 0.81), and ICU length of stay among survivors (aHR = 1.07 [0.87; 1.31], p = 0.53).</p><p><strong>Conclusions: </strong>Including aminoglycosides in the empirical antibiotic therapy did not significantly improve 30-day survival in patients admitted to the ICU for urosepsis. However, the use of aminoglycosides was not associated with worse renal outcomes.</p>\",\"PeriodicalId\":7966,\"journal\":{\"name\":\"Annals of Intensive Care\",\"volume\":\"15 1\",\"pages\":\"52\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2025-04-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11992283/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13613-025-01469-5\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01469-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:目前推荐β -内酰胺和氨基糖苷联合治疗尿脓毒症。肾毒性是氨基糖苷类药物最常见的不良反应,急性肾损伤(AKI)对感染性休克的预后有重要影响。本研究旨在评估有或没有氨基糖苷的经经验抗生素治疗对重症监护病房(ICU)尿脓毒症患者的生存和肾脏预后的影响。方法:这项多中心、回顾性、比较研究纳入了2015年1月至2022年5月期间在巴黎援助Publique-Hôpitaux (APHP)的三所大学医院的四所ICU中因尿脓毒症或脓毒性休克而入院的所有成年人。主要终点是ICU入院后第30天的死亡率。次要终点包括肾脏缺乏恢复,需要新的肾脏替代治疗(RRT),第30天的主要肾脏不良事件(MAKE 30)和ICU住院时间。使用倾向得分加权考虑了指征的混淆。结果:共纳入580例患者,中位年龄69岁(四分位数间:58 ~ 77岁),男性53.6%。总体而言,335名患者(57.8%)在入院时发生脓毒性休克,448名患者(79.2%)有AKI。579例(99.8%)患者接受β -内酰胺作为经验治疗(含(n = 444)或不含(n = 136)氨基糖苷)。总的30天死亡率为10.5%(61/580)。倾向评分加权后,接受氨基糖苷类药物治疗的患者死亡率为7.7%(7/91),而未接受氨基糖苷类药物治疗的患者死亡率为12.1%(11/91)(校正风险比(aHR) = 0.65 [0.35;1.23], p = 0.19)。在第30天肾脏恢复不足方面,两组无显著差异(aHR = 0.88 [0.49;1.58], p = 0.67),需要在30天内进行新的RRT (aHR = 1.01 [0.54;1.88], p = 0.97), MAKE 30 (aHR = 0.94 [0.60;1.50], p = 0.81),幸存者的ICU住院时间(aHR = 1.07 [0.87;1.31], p = 0.53)。结论:在经验抗生素治疗中加入氨基糖苷类药物并不能显著提高ICU尿脓毒症患者的30天生存率。然而,氨基糖苷类药物的使用与肾脏预后不相关。
Impact of aminoglycosides on survival rate and renal outcomes in patients with urosepsis: a multicenter retrospective study.
Background: Combination therapy with a beta-lactam and an aminoglycoside is currently recommended for the empirical treatment of urosepsis. Nephrotoxicity is the most common adverse effect of aminoglycosides and acute kidney injury (AKI) has a significant prognostic impact in septic shock. This study aimed to evaluate the impact of empirical antibiotic therapy with or without an aminoglycoside on survival and renal outcomes in patients admitted to the intensive care unit (ICU) with urosepsis.
Methods: This multicenter, retrospective, comparative study included all adults admitted to the ICU for urinary sepsis or septic shock between January 2015 and May 2022 in four ICUs of three university hospitals within the Assistance Publique-Hôpitaux de Paris (APHP). The primary outcome was mortality on day 30 after ICU admission. Secondary endpoints included the lack of renal recovery, the need for new renal replacement therapy (RRT), the Major Adverse Kidney Events at day 30 (MAKE 30) and ICU length of stay. Confounding by indication was taken into account using propensity score weighting.
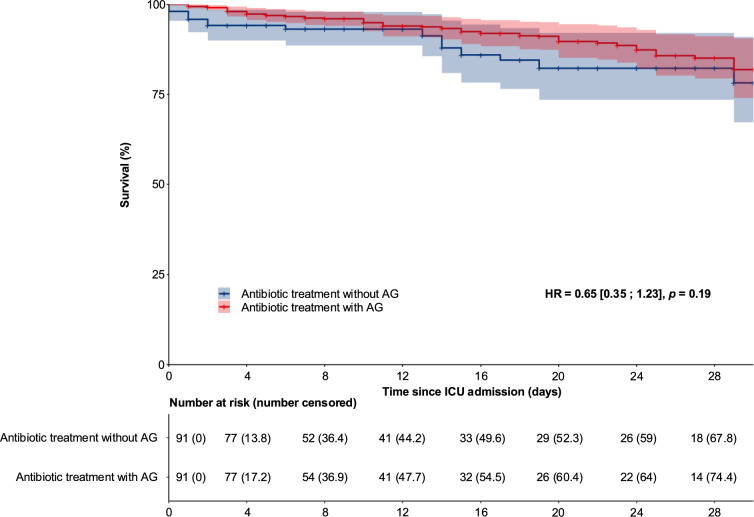
Results: A total of 580 patients were included, median age was 69 years (interquartile: 58-77) and 53.6% were male. Overall, 335 patients (57.8%) were in septic shock and 448 (79.2%) had AKI on admission. A total of 579 patients (99.8%) received a beta-lactam as empirical therapy (with (n = 444) or without (n = 136) aminoglycosides). The overall 30-day mortality rate was 10.5% (61/580). After propensity score weighting, the mortality rate in patients receiving aminoglycosides was 7.7% (7/91) compared to 12.1% (11/91) in those not receiving aminoglycosides (adjusted hazard ratio (aHR) = 0.65 [0.35; 1.23], p = 0.19). No significant differences were found in the lack of renal recovery at day 30 (aHR = 0.88 [0.49; 1.58], p = 0.67), the need for new RRT within 30 days (aHR = 1.01 [0.54; 1.88], p = 0.97), MAKE 30 (aHR = 0.94 [0.60; 1.50], p = 0.81), and ICU length of stay among survivors (aHR = 1.07 [0.87; 1.31], p = 0.53).
Conclusions: Including aminoglycosides in the empirical antibiotic therapy did not significantly improve 30-day survival in patients admitted to the ICU for urosepsis. However, the use of aminoglycosides was not associated with worse renal outcomes.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


