Claudia Dziegielewski, Sarang Gupta, Julia Lombardi, Erin Kelly, Jeffrey D McCurdy, Richmond Sy, Nav Saloojee, Tim Ramsay, Michael Pugliese, Jahanara Begum, Eric I Benchimol, Sanjay K Murthy
{"title":"溃疡性结肠炎成人患者90天再住院风险分层的多变量预测模型","authors":"Claudia Dziegielewski, Sarang Gupta, Julia Lombardi, Erin Kelly, Jeffrey D McCurdy, Richmond Sy, Nav Saloojee, Tim Ramsay, Michael Pugliese, Jahanara Begum, Eric I Benchimol, Sanjay K Murthy","doi":"10.1093/jcag/gwae054","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Individuals with ulcerative colitis (UC) are frequently re-hospitalized for persistent or recurrent severe disease flares. Accurate prediction of the risk of early re-hospitalization at the time of discharge could promote targeted outpatient interventions to reduce this risk.</p><p><strong>Methods: </strong>We conducted a retrospective study in adults with UC admitted to The Ottawa Hospital between 2009 and 2016 for an acute UC-related indication. We ascertained candidate demographic, clinical, and health services predictors through medical records and administrative health databases. We derived and bootstrap validated a multivariable logistic regression model of 90-day UC-related re-hospitalization risk. We chose a probability cut point that maximized Youden's index to differentiate high-risk from low-risk individuals and assessed model performance.</p><p><strong>Results: </strong>Among 248 UC-related hospitalizations, there were 27 (10.9%) re-hospitalizations within 90 days of discharge. Our multivariable model identified gastroenterologist consultation within the prior year (adjusted odds ratio [aOR] 0.11, 95% confidence interval [CI], 0.04-0.39), male sex (aOR 3.27, 95% CI, 1.33-8.05), length of stay (OR 0.94, 95% CI, 0.88-1.01), and narcotic prescription at discharge (OR 1.96, 95% CI, 0.73-5.27) as significant predictors of 90-day re-hospitalization. The optimism-corrected <i>c</i>-statistic value was 0.78, and the goodness-of-fit test <i>P</i>-value was .09. The chosen probability cut point produced a sensitivity of 77.8%, specificity of 80.9%, positive predictive value (PPV) of 33.0%, and negative predictive value (NPV) of 96.7% in the derivation cohort.</p><p><strong>Conclusions: </strong>A limited set of variables accessible at the point of hospital discharge can reasonably discriminate re-hospitalization risk among individuals with UC. Future studies are required to validate our findings.</p>","PeriodicalId":17263,"journal":{"name":"Journal of the Canadian Association of Gastroenterology","volume":"8 2","pages":"76-82"},"PeriodicalIF":2.7000,"publicationDate":"2025-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11991872/pdf/","citationCount":"0","resultStr":"{\"title\":\"A multivariable prediction model to stratify risk of 90-day rehospitalization among adults with ulcerative colitis.\",\"authors\":\"Claudia Dziegielewski, Sarang Gupta, Julia Lombardi, Erin Kelly, Jeffrey D McCurdy, Richmond Sy, Nav Saloojee, Tim Ramsay, Michael Pugliese, Jahanara Begum, Eric I Benchimol, Sanjay K Murthy\",\"doi\":\"10.1093/jcag/gwae054\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Individuals with ulcerative colitis (UC) are frequently re-hospitalized for persistent or recurrent severe disease flares. Accurate prediction of the risk of early re-hospitalization at the time of discharge could promote targeted outpatient interventions to reduce this risk.</p><p><strong>Methods: </strong>We conducted a retrospective study in adults with UC admitted to The Ottawa Hospital between 2009 and 2016 for an acute UC-related indication. We ascertained candidate demographic, clinical, and health services predictors through medical records and administrative health databases. We derived and bootstrap validated a multivariable logistic regression model of 90-day UC-related re-hospitalization risk. We chose a probability cut point that maximized Youden's index to differentiate high-risk from low-risk individuals and assessed model performance.</p><p><strong>Results: </strong>Among 248 UC-related hospitalizations, there were 27 (10.9%) re-hospitalizations within 90 days of discharge. Our multivariable model identified gastroenterologist consultation within the prior year (adjusted odds ratio [aOR] 0.11, 95% confidence interval [CI], 0.04-0.39), male sex (aOR 3.27, 95% CI, 1.33-8.05), length of stay (OR 0.94, 95% CI, 0.88-1.01), and narcotic prescription at discharge (OR 1.96, 95% CI, 0.73-5.27) as significant predictors of 90-day re-hospitalization. The optimism-corrected <i>c</i>-statistic value was 0.78, and the goodness-of-fit test <i>P</i>-value was .09. The chosen probability cut point produced a sensitivity of 77.8%, specificity of 80.9%, positive predictive value (PPV) of 33.0%, and negative predictive value (NPV) of 96.7% in the derivation cohort.</p><p><strong>Conclusions: </strong>A limited set of variables accessible at the point of hospital discharge can reasonably discriminate re-hospitalization risk among individuals with UC. Future studies are required to validate our findings.</p>\",\"PeriodicalId\":17263,\"journal\":{\"name\":\"Journal of the Canadian Association of Gastroenterology\",\"volume\":\"8 2\",\"pages\":\"76-82\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-01-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11991872/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Canadian Association of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jcag/gwae054\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Canadian Association of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jcag/gwae054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A multivariable prediction model to stratify risk of 90-day rehospitalization among adults with ulcerative colitis.
Background: Individuals with ulcerative colitis (UC) are frequently re-hospitalized for persistent or recurrent severe disease flares. Accurate prediction of the risk of early re-hospitalization at the time of discharge could promote targeted outpatient interventions to reduce this risk.
Methods: We conducted a retrospective study in adults with UC admitted to The Ottawa Hospital between 2009 and 2016 for an acute UC-related indication. We ascertained candidate demographic, clinical, and health services predictors through medical records and administrative health databases. We derived and bootstrap validated a multivariable logistic regression model of 90-day UC-related re-hospitalization risk. We chose a probability cut point that maximized Youden's index to differentiate high-risk from low-risk individuals and assessed model performance.
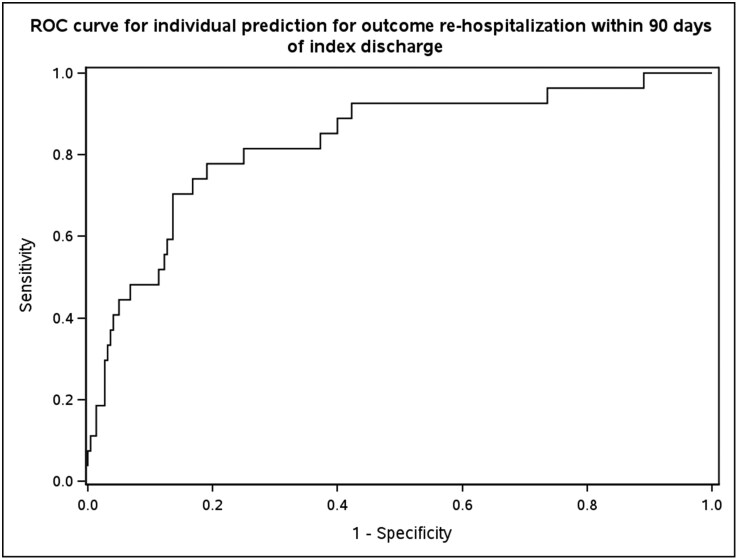
Results: Among 248 UC-related hospitalizations, there were 27 (10.9%) re-hospitalizations within 90 days of discharge. Our multivariable model identified gastroenterologist consultation within the prior year (adjusted odds ratio [aOR] 0.11, 95% confidence interval [CI], 0.04-0.39), male sex (aOR 3.27, 95% CI, 1.33-8.05), length of stay (OR 0.94, 95% CI, 0.88-1.01), and narcotic prescription at discharge (OR 1.96, 95% CI, 0.73-5.27) as significant predictors of 90-day re-hospitalization. The optimism-corrected c-statistic value was 0.78, and the goodness-of-fit test P-value was .09. The chosen probability cut point produced a sensitivity of 77.8%, specificity of 80.9%, positive predictive value (PPV) of 33.0%, and negative predictive value (NPV) of 96.7% in the derivation cohort.
Conclusions: A limited set of variables accessible at the point of hospital discharge can reasonably discriminate re-hospitalization risk among individuals with UC. Future studies are required to validate our findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


