Shinichi Fukuhara, Taichi Suzuki, G Michael Deeb, Gorav Ailawadi, Himanshu J Patel, Bo Yang
{"title":"根据原始风险特征分层的TAVR外植体的临床结果:来自110例TAVR外植体的见解","authors":"Shinichi Fukuhara, Taichi Suzuki, G Michael Deeb, Gorav Ailawadi, Himanshu J Patel, Bo Yang","doi":"10.21037/acs-2024-etavr-0104","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reoperations after transcatheter aortic valve replacement (TAVR) are increasingly reported with consistently poor outcomes. This study aimed to analyze clinical outcomes of TAVR explantation stratified by the original risk profile at the time of TAVR.</p><p><strong>Methods: </strong>We reviewed our single institutional series of 110 consecutive patients who underwent TAVR explant between 2013 and 2024. This cohort was stratified into low-risk (n=35), intermediate-risk (n=35), and high/extreme-risk (n=40) categories based on the original risk profile.</p><p><strong>Results: </strong>Low-risk patients began to appear in 2018. By 2021, the number of low/intermediate-risk patients surpassed that of the high/extreme-risk group. Balloon-expandable valves were predominantly used in the low-risk group, whereas chronic kidney disease was more prevalent in the other groups. The majority of patients in each group had either structural valve deterioration (SVD) and/or non-SVD as the primary failure mechanism, with endocarditis accounting for 20% or less. Cardiopulmonary bypass/aortic cross-clamp times were longest in the high-/extreme-risk group. Overall, 75 (68.2%) patients underwent a concomitant procedure during TAVR explant, most commonly an aortic (n=39; 52.0%) and a mitral procedure (n=29; 38.7%). The high/extreme-risk group had the highest rates of concomitant procedures. Operative mortality improved significantly over time, dropping from 27.3% in Era 1 (2013-2017) to 5.6% in Era 3 (2022-2024) (P=0.049). The operative and one-year mortality rates were 8.6%, 8.6%, and 7.5% (P=0.98), and 17.1%, 8.6%, and 17.5% (P=0.48) in the low-, intermediate-, and high-/extreme-risk group, respectively. Conversely, the observed-to-expected mortality ratio (O/E ratio) was highest in the low-risk group (2.8 <i>vs.</i> 1.0 <i>vs.</i> 0.8; P<0.001).</p><p><strong>Conclusions: </strong>Low-risk patients are emerging as the predominant group requiring TAVR explant. Despite the procedural simplicity and lower-risk profile, the operative mortality was comparable to higher-risk groups, and the O/E ratio was significantly higher in the low-risk group. Thoughtful reconsideration of the TAVR-first approach may be warranted for this population.</p>","PeriodicalId":8067,"journal":{"name":"Annals of cardiothoracic surgery","volume":"14 2","pages":"122-130"},"PeriodicalIF":3.1000,"publicationDate":"2025-03-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12013758/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical outcomes of TAVR explant stratified by original risk profile: insights from 110 TAVR explants.\",\"authors\":\"Shinichi Fukuhara, Taichi Suzuki, G Michael Deeb, Gorav Ailawadi, Himanshu J Patel, Bo Yang\",\"doi\":\"10.21037/acs-2024-etavr-0104\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Reoperations after transcatheter aortic valve replacement (TAVR) are increasingly reported with consistently poor outcomes. This study aimed to analyze clinical outcomes of TAVR explantation stratified by the original risk profile at the time of TAVR.</p><p><strong>Methods: </strong>We reviewed our single institutional series of 110 consecutive patients who underwent TAVR explant between 2013 and 2024. This cohort was stratified into low-risk (n=35), intermediate-risk (n=35), and high/extreme-risk (n=40) categories based on the original risk profile.</p><p><strong>Results: </strong>Low-risk patients began to appear in 2018. By 2021, the number of low/intermediate-risk patients surpassed that of the high/extreme-risk group. Balloon-expandable valves were predominantly used in the low-risk group, whereas chronic kidney disease was more prevalent in the other groups. The majority of patients in each group had either structural valve deterioration (SVD) and/or non-SVD as the primary failure mechanism, with endocarditis accounting for 20% or less. Cardiopulmonary bypass/aortic cross-clamp times were longest in the high-/extreme-risk group. Overall, 75 (68.2%) patients underwent a concomitant procedure during TAVR explant, most commonly an aortic (n=39; 52.0%) and a mitral procedure (n=29; 38.7%). The high/extreme-risk group had the highest rates of concomitant procedures. Operative mortality improved significantly over time, dropping from 27.3% in Era 1 (2013-2017) to 5.6% in Era 3 (2022-2024) (P=0.049). The operative and one-year mortality rates were 8.6%, 8.6%, and 7.5% (P=0.98), and 17.1%, 8.6%, and 17.5% (P=0.48) in the low-, intermediate-, and high-/extreme-risk group, respectively. Conversely, the observed-to-expected mortality ratio (O/E ratio) was highest in the low-risk group (2.8 <i>vs.</i> 1.0 <i>vs.</i> 0.8; P<0.001).</p><p><strong>Conclusions: </strong>Low-risk patients are emerging as the predominant group requiring TAVR explant. Despite the procedural simplicity and lower-risk profile, the operative mortality was comparable to higher-risk groups, and the O/E ratio was significantly higher in the low-risk group. Thoughtful reconsideration of the TAVR-first approach may be warranted for this population.</p>\",\"PeriodicalId\":8067,\"journal\":{\"name\":\"Annals of cardiothoracic surgery\",\"volume\":\"14 2\",\"pages\":\"122-130\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-03-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12013758/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of cardiothoracic surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/acs-2024-etavr-0104\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of cardiothoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/acs-2024-etavr-0104","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:经导管主动脉瓣置换术(TAVR)后再手术的报道越来越多,结果一直很差。本研究旨在分析TAVR移植的临床结果,根据TAVR移植时的原始风险概况进行分层。方法:我们回顾了2013年至2024年间接受TAVR移植的110例连续患者的单一机构系列。该队列根据原始风险概况分为低风险(n=35)、中风险(n=35)和高风险/极端风险(n=40)三类。结果:2018年开始出现低危患者。到2021年,低/中等风险患者的数量超过了高/极端风险组。可膨胀球囊瓣膜主要用于低风险组,而慢性肾脏疾病在其他组中更为普遍。各组患者以结构性瓣膜恶化(SVD)和/或非SVD为主要衰竭机制,心内膜炎占20%或更少。高危/极危组体外循环/主动脉交叉夹持时间最长。总体而言,75例(68.2%)患者在TAVR移植期间接受了伴随手术,最常见的是主动脉(n=39;52.0%)和二尖瓣手术(n=29;38.7%)。高/极端风险组的伴随手术率最高。手术死亡率随着时间的推移显著改善,从第1时代(2013-2017年)的27.3%下降到第3时代(2022-2024年)的5.6% (P=0.049)。低、中、高/极危组的手术死亡率和一年死亡率分别为8.6%、8.6%和7.5% (P=0.98), 17.1%、8.6%和17.5% (P=0.48)。相反,低危组的观察到的预期死亡率(O/E比)最高(2.8 vs 1.0 vs 0.8;结论:低危患者正在成为TAVR移植的主要需求群体。尽管手术简单且风险较低,但手术死亡率与高危组相当,且低危组的O/E比明显较高。对于这一人群,可能需要对TAVR-first方法进行深思熟虑的重新考虑。
Clinical outcomes of TAVR explant stratified by original risk profile: insights from 110 TAVR explants.
Background: Reoperations after transcatheter aortic valve replacement (TAVR) are increasingly reported with consistently poor outcomes. This study aimed to analyze clinical outcomes of TAVR explantation stratified by the original risk profile at the time of TAVR.
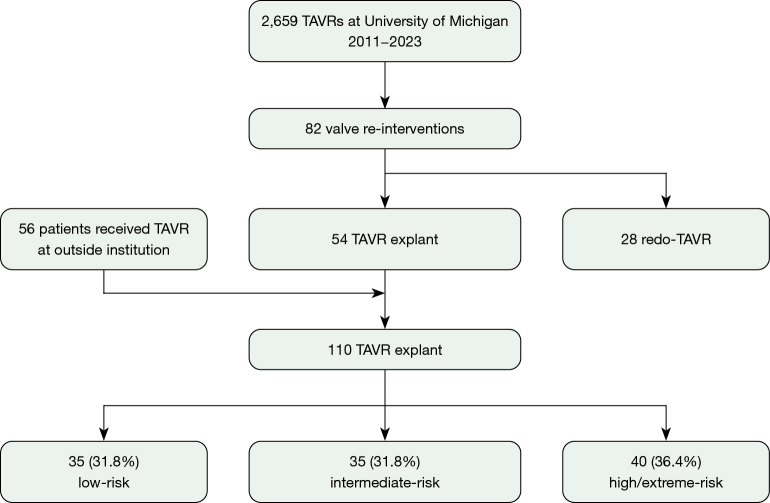
Methods: We reviewed our single institutional series of 110 consecutive patients who underwent TAVR explant between 2013 and 2024. This cohort was stratified into low-risk (n=35), intermediate-risk (n=35), and high/extreme-risk (n=40) categories based on the original risk profile.
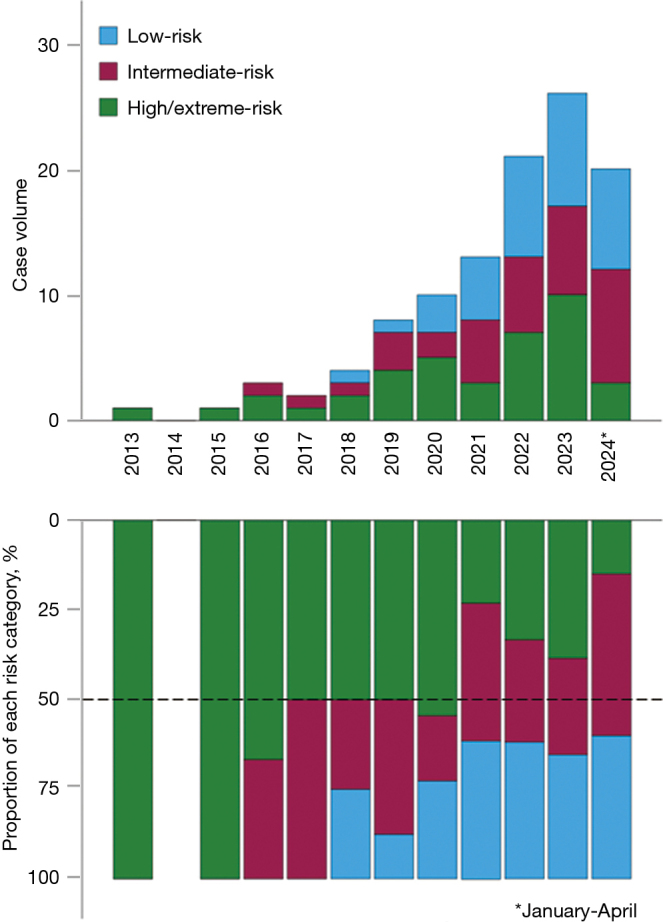
Results: Low-risk patients began to appear in 2018. By 2021, the number of low/intermediate-risk patients surpassed that of the high/extreme-risk group. Balloon-expandable valves were predominantly used in the low-risk group, whereas chronic kidney disease was more prevalent in the other groups. The majority of patients in each group had either structural valve deterioration (SVD) and/or non-SVD as the primary failure mechanism, with endocarditis accounting for 20% or less. Cardiopulmonary bypass/aortic cross-clamp times were longest in the high-/extreme-risk group. Overall, 75 (68.2%) patients underwent a concomitant procedure during TAVR explant, most commonly an aortic (n=39; 52.0%) and a mitral procedure (n=29; 38.7%). The high/extreme-risk group had the highest rates of concomitant procedures. Operative mortality improved significantly over time, dropping from 27.3% in Era 1 (2013-2017) to 5.6% in Era 3 (2022-2024) (P=0.049). The operative and one-year mortality rates were 8.6%, 8.6%, and 7.5% (P=0.98), and 17.1%, 8.6%, and 17.5% (P=0.48) in the low-, intermediate-, and high-/extreme-risk group, respectively. Conversely, the observed-to-expected mortality ratio (O/E ratio) was highest in the low-risk group (2.8 vs. 1.0 vs. 0.8; P<0.001).
Conclusions: Low-risk patients are emerging as the predominant group requiring TAVR explant. Despite the procedural simplicity and lower-risk profile, the operative mortality was comparable to higher-risk groups, and the O/E ratio was significantly higher in the low-risk group. Thoughtful reconsideration of the TAVR-first approach may be warranted for this population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


