Muhilan Senthilkumar, Satyen Parida, Priya Rudingwa, Raja Selvaraj
{"title":"胸肌平面阻滞与肋间神经阻滞联合局部浸润镇痛在心脏植入式电子装置植入中的比较——一项随机对照试验。","authors":"Muhilan Senthilkumar, Satyen Parida, Priya Rudingwa, Raja Selvaraj","doi":"10.4103/aca.aca_164_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac implantable electronic device (CIED) implantation rates have increased exponentially over the past few decades. Limited options are available for pain-free courses during this procedure. Traditionally, local infiltration with conscious sedation is being used. The pectoral nerves (PECS) block has been evaluated for its analgesic efficacy in breast surgeries. Our study assessed the effectiveness of combined PECS 1 block and intercostal nerve block over local infiltration as an analgesic technique during CIED implantations.</p><p><strong>Method: </strong>In this randomized controlled trial, 70 ASA 2 and 3 patients in the age group of 18-75 years scheduled for CIED implantation were randomized into two groups. Group A received local infiltration with 14 ml of 0.375% ropivacaine, and group B received a combined PECS 1 block (10 ml) and intercostal nerve block (4 ml) under ultrasound guidance. Additional lignocaine 1% as 2 ml aliquots was given as rescue during the procedure. We noted the frequency and timing of aliquots. The pain was assessed at 1, 2, 4, 8 and 24 hours post procedure, and intravenous paracetamol was given if the numeric rating scale (NRS) was more than 3. The total paracetamol required and the mean duration of hospital stay were noted for both groups.</p><p><strong>Results: </strong>There was a statistically significant decrease in NRS scores at the initial five steps of the procedure in group B except at skin closure, P value = 0.044. The time for the first demand for analgesia was significantly prolonged in group B with 39.6 ± 15.9 vs 19.6 ± 15.1 minutes in the local infiltration group, respectively, with P value = 0.001. Mean fentanyl requirement during the procedure was significantly lower in B (30.4 ± 10.4 mcg vs 50.7 ± 17.7 mcg) when compared to group A, P value < 0.001, and so was the paracetamol requirement in the postprocedure period, P value = 0.003. The postprocedure pain scores and the duration of hospital stay were comparable for both.</p><p><strong>Conclusion: </strong>Combined PECS 1 and intercostal nerve block in place of traditional local infiltration significantly reduced NRS score and rescue drug requirement during the procedure. It is a suitable option for these patients.</p>","PeriodicalId":7997,"journal":{"name":"Annals of Cardiac Anaesthesia","volume":"28 2","pages":"170-175"},"PeriodicalIF":1.3000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058071/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of Combined Pectoralis Plane Block and Intercostal Nerve Block with Local Infiltration Analgesia in Patients Undergoing Cardiac Implantable Electronic Device Implantation - A Randomized Controlled Trial.\",\"authors\":\"Muhilan Senthilkumar, Satyen Parida, Priya Rudingwa, Raja Selvaraj\",\"doi\":\"10.4103/aca.aca_164_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiac implantable electronic device (CIED) implantation rates have increased exponentially over the past few decades. Limited options are available for pain-free courses during this procedure. Traditionally, local infiltration with conscious sedation is being used. The pectoral nerves (PECS) block has been evaluated for its analgesic efficacy in breast surgeries. Our study assessed the effectiveness of combined PECS 1 block and intercostal nerve block over local infiltration as an analgesic technique during CIED implantations.</p><p><strong>Method: </strong>In this randomized controlled trial, 70 ASA 2 and 3 patients in the age group of 18-75 years scheduled for CIED implantation were randomized into two groups. Group A received local infiltration with 14 ml of 0.375% ropivacaine, and group B received a combined PECS 1 block (10 ml) and intercostal nerve block (4 ml) under ultrasound guidance. Additional lignocaine 1% as 2 ml aliquots was given as rescue during the procedure. We noted the frequency and timing of aliquots. The pain was assessed at 1, 2, 4, 8 and 24 hours post procedure, and intravenous paracetamol was given if the numeric rating scale (NRS) was more than 3. The total paracetamol required and the mean duration of hospital stay were noted for both groups.</p><p><strong>Results: </strong>There was a statistically significant decrease in NRS scores at the initial five steps of the procedure in group B except at skin closure, P value = 0.044. The time for the first demand for analgesia was significantly prolonged in group B with 39.6 ± 15.9 vs 19.6 ± 15.1 minutes in the local infiltration group, respectively, with P value = 0.001. Mean fentanyl requirement during the procedure was significantly lower in B (30.4 ± 10.4 mcg vs 50.7 ± 17.7 mcg) when compared to group A, P value < 0.001, and so was the paracetamol requirement in the postprocedure period, P value = 0.003. The postprocedure pain scores and the duration of hospital stay were comparable for both.</p><p><strong>Conclusion: </strong>Combined PECS 1 and intercostal nerve block in place of traditional local infiltration significantly reduced NRS score and rescue drug requirement during the procedure. It is a suitable option for these patients.</p>\",\"PeriodicalId\":7997,\"journal\":{\"name\":\"Annals of Cardiac Anaesthesia\",\"volume\":\"28 2\",\"pages\":\"170-175\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058071/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Cardiac Anaesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/aca.aca_164_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Cardiac Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aca.aca_164_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Comparison of Combined Pectoralis Plane Block and Intercostal Nerve Block with Local Infiltration Analgesia in Patients Undergoing Cardiac Implantable Electronic Device Implantation - A Randomized Controlled Trial.
Background: Cardiac implantable electronic device (CIED) implantation rates have increased exponentially over the past few decades. Limited options are available for pain-free courses during this procedure. Traditionally, local infiltration with conscious sedation is being used. The pectoral nerves (PECS) block has been evaluated for its analgesic efficacy in breast surgeries. Our study assessed the effectiveness of combined PECS 1 block and intercostal nerve block over local infiltration as an analgesic technique during CIED implantations.
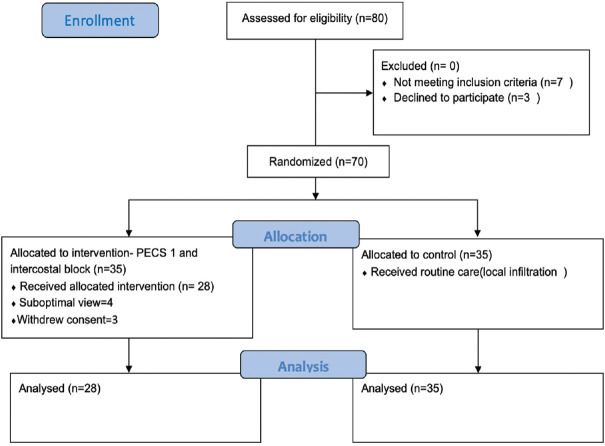
Method: In this randomized controlled trial, 70 ASA 2 and 3 patients in the age group of 18-75 years scheduled for CIED implantation were randomized into two groups. Group A received local infiltration with 14 ml of 0.375% ropivacaine, and group B received a combined PECS 1 block (10 ml) and intercostal nerve block (4 ml) under ultrasound guidance. Additional lignocaine 1% as 2 ml aliquots was given as rescue during the procedure. We noted the frequency and timing of aliquots. The pain was assessed at 1, 2, 4, 8 and 24 hours post procedure, and intravenous paracetamol was given if the numeric rating scale (NRS) was more than 3. The total paracetamol required and the mean duration of hospital stay were noted for both groups.
Results: There was a statistically significant decrease in NRS scores at the initial five steps of the procedure in group B except at skin closure, P value = 0.044. The time for the first demand for analgesia was significantly prolonged in group B with 39.6 ± 15.9 vs 19.6 ± 15.1 minutes in the local infiltration group, respectively, with P value = 0.001. Mean fentanyl requirement during the procedure was significantly lower in B (30.4 ± 10.4 mcg vs 50.7 ± 17.7 mcg) when compared to group A, P value < 0.001, and so was the paracetamol requirement in the postprocedure period, P value = 0.003. The postprocedure pain scores and the duration of hospital stay were comparable for both.
Conclusion: Combined PECS 1 and intercostal nerve block in place of traditional local infiltration significantly reduced NRS score and rescue drug requirement during the procedure. It is a suitable option for these patients.
期刊介绍:
Annals of Cardiac Anaesthesia (ACA) is the official journal of the Indian Association of Cardiovascular Thoracic Anaesthesiologists. The journal is indexed with PubMed/MEDLINE, Excerpta Medica/EMBASE, IndMed and MedInd. The journal’s full text is online at www.annals.in. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in ACA. Authors do not have to pay for submission, processing or publication of articles in ACA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


