Matthew G Wilson, Folkert W Asselbergs, Nausheen Saleem, Lelia Jeilani, David Brealey, Matthew R Sydes, Steve Harris
{"title":"将研究行为数字化整合到临床护理:PROSPECTOR随机可行性研究的结果。","authors":"Matthew G Wilson, Folkert W Asselbergs, Nausheen Saleem, Lelia Jeilani, David Brealey, Matthew R Sydes, Steve Harris","doi":"10.1136/bmjebm-2024-113081","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the feasibility of conducting a clinically integrated randomised comparative effectiveness trial using digital clinical trial infrastructure within an electronic patient record (EPR).</p><p><strong>Design: </strong>A mixed-methods, unblinded, feasibility study of digital clinical trial system incorporating testing of two designs of electronic point-of-care randomisation prompt.</p><p><strong>Setting: </strong>The study was conducted at University College London Hospitals NHS Trust between March and November 2022. The study used a real clinical research question for context, comparing liberal vs restrictive strategies for magnesium supplementation to prevent new-onset atrial fibrillation in critical care.</p><p><strong>Participants: </strong>Adult patients undergoing elective, non-cardiac surgical procedures expecting postoperative admission to critical care were recruited.</p><p><strong>Interventions: </strong>A digital trial system screened participants continuously against eligibility criteria. Participants were automatically randomised (1:1) to (1) magnesium supplementation strategy and (2) one of two electronic randomisation prompt designs (nudge or preference).Electronic point-of-care randomisation prompts displayed to clinicians at regular intervals, inviting them to follow a randomised magnesium supplementation suggestion.</p><p><strong>Main outcome measures: </strong>The primary outcome measure was a composite determination of study design feasibility (including recruitment, technical performance and concordance between the randomised suggestion and the observed clinician action).</p><p><strong>Results: </strong>23 patients were recruited and 11 successfully randomised. The implemented digital systems for automated eligibility screening, randomisation, data collection and follow-up demonstrated technical feasibility. 47 electronic point-of-care randomisation prompts successfully deployed across 11 patients. Clinician actions were concordant with randomised suggestions in 32 prompts (68%).Technical and implementational barriers to delivering the electronic point-of-care randomisation prompts were identified. Patients were followed up to 30 days following discharge from hospital, with no serious adverse events attributable to participation identified.There was insufficient data to make a quantitative determination on the superiority of either prompt design. Clinician feedback suggested the simplified design (nudge) had greater utility.</p><p><strong>Conclusions: </strong>This study demonstrates that digitally embedding clinical trial infrastructure into a site-level EPR and integrating conduct into clinical care is safe and feasible. Future work will focus on improving and expanding the integrated digital trial design across multiple centres.</p><p><strong>Trial registration number: </strong>NCT05149820.</p>","PeriodicalId":9059,"journal":{"name":"BMJ Evidence-Based Medicine","volume":" ","pages":"323-332"},"PeriodicalIF":7.6000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12505030/pdf/","citationCount":"0","resultStr":"{\"title\":\"Digital integration of research conduct into clinical care: results of the PROSPECTOR randomised feasibility study.\",\"authors\":\"Matthew G Wilson, Folkert W Asselbergs, Nausheen Saleem, Lelia Jeilani, David Brealey, Matthew R Sydes, Steve Harris\",\"doi\":\"10.1136/bmjebm-2024-113081\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate the feasibility of conducting a clinically integrated randomised comparative effectiveness trial using digital clinical trial infrastructure within an electronic patient record (EPR).</p><p><strong>Design: </strong>A mixed-methods, unblinded, feasibility study of digital clinical trial system incorporating testing of two designs of electronic point-of-care randomisation prompt.</p><p><strong>Setting: </strong>The study was conducted at University College London Hospitals NHS Trust between March and November 2022. The study used a real clinical research question for context, comparing liberal vs restrictive strategies for magnesium supplementation to prevent new-onset atrial fibrillation in critical care.</p><p><strong>Participants: </strong>Adult patients undergoing elective, non-cardiac surgical procedures expecting postoperative admission to critical care were recruited.</p><p><strong>Interventions: </strong>A digital trial system screened participants continuously against eligibility criteria. Participants were automatically randomised (1:1) to (1) magnesium supplementation strategy and (2) one of two electronic randomisation prompt designs (nudge or preference).Electronic point-of-care randomisation prompts displayed to clinicians at regular intervals, inviting them to follow a randomised magnesium supplementation suggestion.</p><p><strong>Main outcome measures: </strong>The primary outcome measure was a composite determination of study design feasibility (including recruitment, technical performance and concordance between the randomised suggestion and the observed clinician action).</p><p><strong>Results: </strong>23 patients were recruited and 11 successfully randomised. The implemented digital systems for automated eligibility screening, randomisation, data collection and follow-up demonstrated technical feasibility. 47 electronic point-of-care randomisation prompts successfully deployed across 11 patients. Clinician actions were concordant with randomised suggestions in 32 prompts (68%).Technical and implementational barriers to delivering the electronic point-of-care randomisation prompts were identified. Patients were followed up to 30 days following discharge from hospital, with no serious adverse events attributable to participation identified.There was insufficient data to make a quantitative determination on the superiority of either prompt design. Clinician feedback suggested the simplified design (nudge) had greater utility.</p><p><strong>Conclusions: </strong>This study demonstrates that digitally embedding clinical trial infrastructure into a site-level EPR and integrating conduct into clinical care is safe and feasible. Future work will focus on improving and expanding the integrated digital trial design across multiple centres.</p><p><strong>Trial registration number: </strong>NCT05149820.</p>\",\"PeriodicalId\":9059,\"journal\":{\"name\":\"BMJ Evidence-Based Medicine\",\"volume\":\" \",\"pages\":\"323-332\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2025-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12505030/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Evidence-Based Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjebm-2024-113081\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Evidence-Based Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjebm-2024-113081","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Digital integration of research conduct into clinical care: results of the PROSPECTOR randomised feasibility study.
Objectives: To evaluate the feasibility of conducting a clinically integrated randomised comparative effectiveness trial using digital clinical trial infrastructure within an electronic patient record (EPR).
Design: A mixed-methods, unblinded, feasibility study of digital clinical trial system incorporating testing of two designs of electronic point-of-care randomisation prompt.
Setting: The study was conducted at University College London Hospitals NHS Trust between March and November 2022. The study used a real clinical research question for context, comparing liberal vs restrictive strategies for magnesium supplementation to prevent new-onset atrial fibrillation in critical care.
Participants: Adult patients undergoing elective, non-cardiac surgical procedures expecting postoperative admission to critical care were recruited.
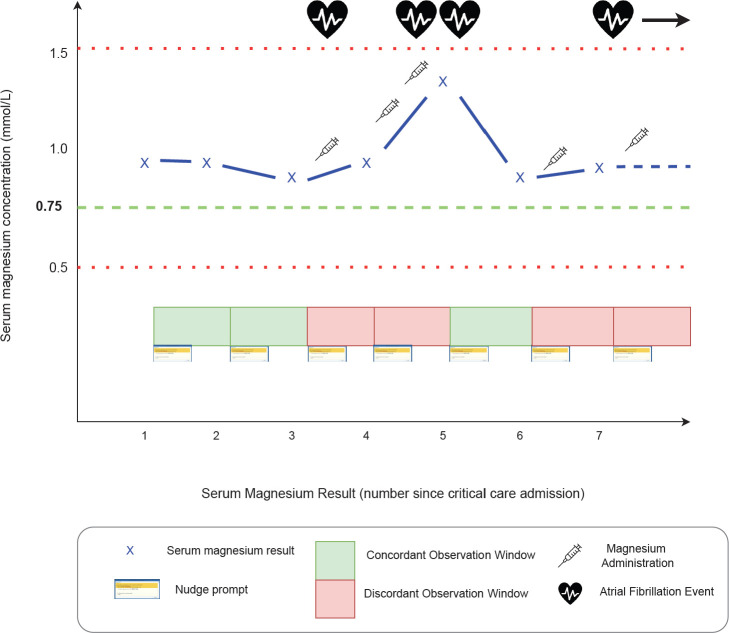
Interventions: A digital trial system screened participants continuously against eligibility criteria. Participants were automatically randomised (1:1) to (1) magnesium supplementation strategy and (2) one of two electronic randomisation prompt designs (nudge or preference).Electronic point-of-care randomisation prompts displayed to clinicians at regular intervals, inviting them to follow a randomised magnesium supplementation suggestion.
Main outcome measures: The primary outcome measure was a composite determination of study design feasibility (including recruitment, technical performance and concordance between the randomised suggestion and the observed clinician action).
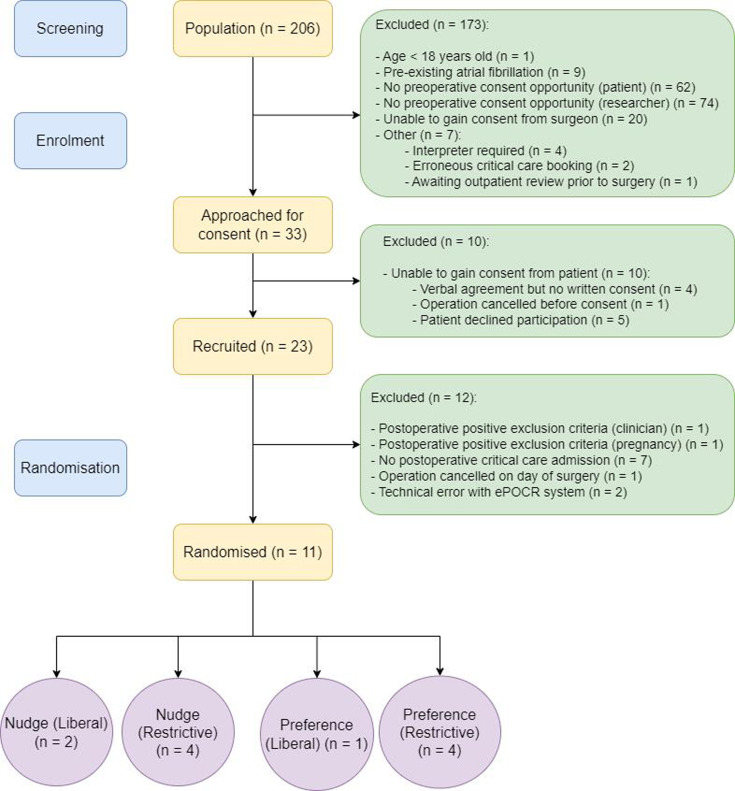
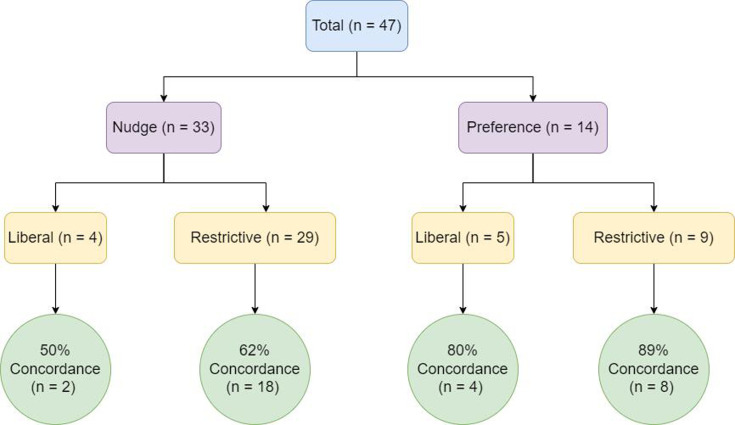
Results: 23 patients were recruited and 11 successfully randomised. The implemented digital systems for automated eligibility screening, randomisation, data collection and follow-up demonstrated technical feasibility. 47 electronic point-of-care randomisation prompts successfully deployed across 11 patients. Clinician actions were concordant with randomised suggestions in 32 prompts (68%).Technical and implementational barriers to delivering the electronic point-of-care randomisation prompts were identified. Patients were followed up to 30 days following discharge from hospital, with no serious adverse events attributable to participation identified.There was insufficient data to make a quantitative determination on the superiority of either prompt design. Clinician feedback suggested the simplified design (nudge) had greater utility.
Conclusions: This study demonstrates that digitally embedding clinical trial infrastructure into a site-level EPR and integrating conduct into clinical care is safe and feasible. Future work will focus on improving and expanding the integrated digital trial design across multiple centres.
期刊介绍:
BMJ Evidence-Based Medicine (BMJ EBM) publishes original evidence-based research, insights and opinions on what matters for health care. We focus on the tools, methods, and concepts that are basic and central to practising evidence-based medicine and deliver relevant, trustworthy and impactful evidence.
BMJ EBM is a Plan S compliant Transformative Journal and adheres to the highest possible industry standards for editorial policies and publication ethics.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


