Shubh Patel, Jiawen Deng, Areeba Zubair, Kiyan Heybati, Shayan Heybati, Oswin Chang, Umaima Abbas, Umair Tahir, Harikrishnaa B Ramaraju, Chi Y Wong, Thanansayan Dhivagaran, Daniel Rayner, Magnus Krever, Tiffany Woelber, Gurukripa N Kowlgi, Harish Ramakrishna
{"title":"镇静与全身麻醉消融室性心律失常:系统回顾和荟萃分析。","authors":"Shubh Patel, Jiawen Deng, Areeba Zubair, Kiyan Heybati, Shayan Heybati, Oswin Chang, Umaima Abbas, Umair Tahir, Harikrishnaa B Ramaraju, Chi Y Wong, Thanansayan Dhivagaran, Daniel Rayner, Magnus Krever, Tiffany Woelber, Gurukripa N Kowlgi, Harish Ramakrishna","doi":"10.4103/aca.aca_229_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>Ventricular arrhythmias (VA), including ventricular tachycardia and fibrillation, are critical cardiac conditions that are often managed by catheter ablation among those unresponsive to pharmacologic therapy. The choice of anesthesia and sedation regimens for VA ablations may impact arrhythmia inducibility and hemodynamic stability, which can affect procedural success and complication rates. This systematic review and meta-analysis aimed to compare the efficacy and safety of sedation versus general anesthesia (GA) among patients undergoing VA ablation. The review was prospectively registered on PROSPERO (CRD42023441553). Database searches were conducted across five major databases from inception to March 9, 2024 to identify randomized trials or observational studies including adult patients undergoing ablations for VA. Screening and data extraction were completed in duplicate. Risk-of-bias assessments were conducted using ROBINS-I as all included studies were observational, and the quality of evidence was evaluated using the GRADE framework. Six observational studies (N = 16,435) were included. No significant differences were found between sedation and GA for total procedure time (MD: -14.16 minutes; 95%CI: -38.61 to 10.29 minutes), arrhythmia non-inducibility (RR: 0.73; 95% CI: 0.33-1.58), acute ablation success (RR: 1.06; 95% CI: 0.65-1.71), or procedural complications (RR: 0.72; 95% CI: 0.28-1.85). However, sedation was associated with significantly lower intraprocedural hemodynamic instability (RR: 0.28; 95% CI: 0.12-0.70). These findings indicate that while sedation and GA have comparable outcomes, sedation may be associated with less hemodynamic instability during VA ablation. However, more high-quality studies are needed to confirm these results.</p>","PeriodicalId":7997,"journal":{"name":"Annals of Cardiac Anaesthesia","volume":"28 2","pages":"119-127"},"PeriodicalIF":1.3000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058075/pdf/","citationCount":"0","resultStr":"{\"title\":\"Sedation Versus General Anesthesia for Ablation of Ventricular Arrhythmias: A Systematic Review and Meta-Analysis.\",\"authors\":\"Shubh Patel, Jiawen Deng, Areeba Zubair, Kiyan Heybati, Shayan Heybati, Oswin Chang, Umaima Abbas, Umair Tahir, Harikrishnaa B Ramaraju, Chi Y Wong, Thanansayan Dhivagaran, Daniel Rayner, Magnus Krever, Tiffany Woelber, Gurukripa N Kowlgi, Harish Ramakrishna\",\"doi\":\"10.4103/aca.aca_229_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Abstract: </strong>Ventricular arrhythmias (VA), including ventricular tachycardia and fibrillation, are critical cardiac conditions that are often managed by catheter ablation among those unresponsive to pharmacologic therapy. The choice of anesthesia and sedation regimens for VA ablations may impact arrhythmia inducibility and hemodynamic stability, which can affect procedural success and complication rates. This systematic review and meta-analysis aimed to compare the efficacy and safety of sedation versus general anesthesia (GA) among patients undergoing VA ablation. The review was prospectively registered on PROSPERO (CRD42023441553). Database searches were conducted across five major databases from inception to March 9, 2024 to identify randomized trials or observational studies including adult patients undergoing ablations for VA. Screening and data extraction were completed in duplicate. Risk-of-bias assessments were conducted using ROBINS-I as all included studies were observational, and the quality of evidence was evaluated using the GRADE framework. Six observational studies (N = 16,435) were included. No significant differences were found between sedation and GA for total procedure time (MD: -14.16 minutes; 95%CI: -38.61 to 10.29 minutes), arrhythmia non-inducibility (RR: 0.73; 95% CI: 0.33-1.58), acute ablation success (RR: 1.06; 95% CI: 0.65-1.71), or procedural complications (RR: 0.72; 95% CI: 0.28-1.85). However, sedation was associated with significantly lower intraprocedural hemodynamic instability (RR: 0.28; 95% CI: 0.12-0.70). These findings indicate that while sedation and GA have comparable outcomes, sedation may be associated with less hemodynamic instability during VA ablation. However, more high-quality studies are needed to confirm these results.</p>\",\"PeriodicalId\":7997,\"journal\":{\"name\":\"Annals of Cardiac Anaesthesia\",\"volume\":\"28 2\",\"pages\":\"119-127\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058075/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Cardiac Anaesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/aca.aca_229_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Cardiac Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aca.aca_229_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Sedation Versus General Anesthesia for Ablation of Ventricular Arrhythmias: A Systematic Review and Meta-Analysis.
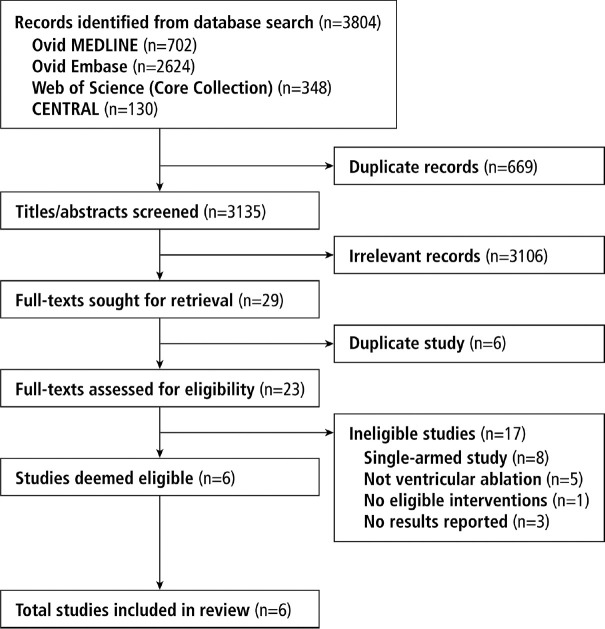
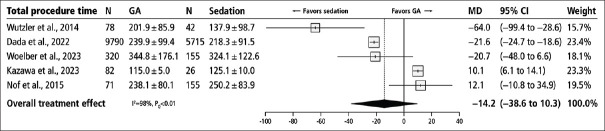
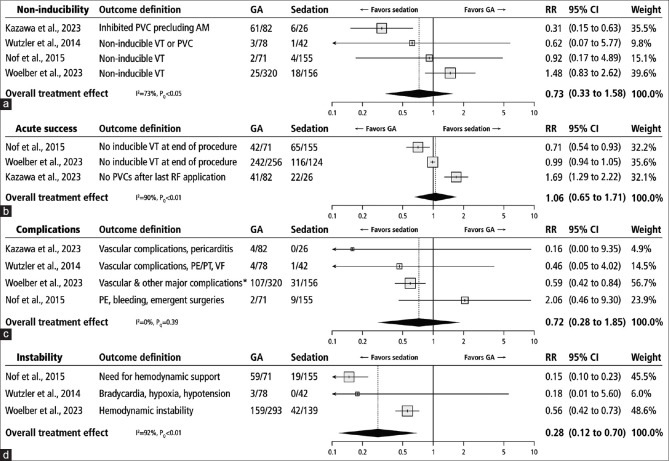
Abstract: Ventricular arrhythmias (VA), including ventricular tachycardia and fibrillation, are critical cardiac conditions that are often managed by catheter ablation among those unresponsive to pharmacologic therapy. The choice of anesthesia and sedation regimens for VA ablations may impact arrhythmia inducibility and hemodynamic stability, which can affect procedural success and complication rates. This systematic review and meta-analysis aimed to compare the efficacy and safety of sedation versus general anesthesia (GA) among patients undergoing VA ablation. The review was prospectively registered on PROSPERO (CRD42023441553). Database searches were conducted across five major databases from inception to March 9, 2024 to identify randomized trials or observational studies including adult patients undergoing ablations for VA. Screening and data extraction were completed in duplicate. Risk-of-bias assessments were conducted using ROBINS-I as all included studies were observational, and the quality of evidence was evaluated using the GRADE framework. Six observational studies (N = 16,435) were included. No significant differences were found between sedation and GA for total procedure time (MD: -14.16 minutes; 95%CI: -38.61 to 10.29 minutes), arrhythmia non-inducibility (RR: 0.73; 95% CI: 0.33-1.58), acute ablation success (RR: 1.06; 95% CI: 0.65-1.71), or procedural complications (RR: 0.72; 95% CI: 0.28-1.85). However, sedation was associated with significantly lower intraprocedural hemodynamic instability (RR: 0.28; 95% CI: 0.12-0.70). These findings indicate that while sedation and GA have comparable outcomes, sedation may be associated with less hemodynamic instability during VA ablation. However, more high-quality studies are needed to confirm these results.
期刊介绍:
Annals of Cardiac Anaesthesia (ACA) is the official journal of the Indian Association of Cardiovascular Thoracic Anaesthesiologists. The journal is indexed with PubMed/MEDLINE, Excerpta Medica/EMBASE, IndMed and MedInd. The journal’s full text is online at www.annals.in. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in ACA. Authors do not have to pay for submission, processing or publication of articles in ACA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


