{"title":"质疑二甲双胍治疗糖尿病周围神经病变的利弊。","authors":"Hiroki Mizukami","doi":"10.1111/jdi.70055","DOIUrl":null,"url":null,"abstract":"<p>Diabetic peripheral neuropathy (DPN) is the most common complication among diabetic patients. Its symptoms include pain, hyperalgesia, hypoalgesia, and paralysis, all of which can significantly reduce patients' quality of life. In DPN, peripheral nerve fibers are affected as early as the prediabetic stage. Currently, no curative treatment has been established. As demonstrated in large clinical trials like the Diabetes Control and Complication Trial, strict glycemic control remains the only proven method to slow the progression of DPN. Consequently, it is crucial to identify which diabetes medications are more effective against neuropathy or, at the very least, do not exacerbate it.</p><p>Experimentally, various antidiabetic drugs—including dipeptidyl peptidase-4 (DPP-4) inhibitors, α-glucosidase inhibitors, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and incretin agonists—have shown therapeutic effects on DPN that are independent of blood glucose improvement<span><sup>1</sup></span>. Among oral antidiabetic agents, metformin is one of the most widely used drugs for diabetes. However, its effects on DPN remain controversial. Several studies have reported that metformin use decreases cobalamin (Vitamin B12) levels while increasing its related metabolite homocysteine and methylmalonic acid. Deficiency in cobalamin and elevated homocysteine and methylmalonic acid levels are known to induce peripheral neuropathy; hence, metformin has been suggested to worsen DPN<span><sup>2</sup></span>. On the other hand, some studies indicate that metformin has no apparent effect on DPN<span><sup>3</sup></span>. Furthermore, other research suggests that while metformin reduces cobalamin levels, it does not influence DPN progression<span><sup>4</sup></span>. As such, the therapeutic effects of metformin on DPN remain contentious.</p><p>In this context, Dhanapalaratnam <i>et al</i>.<span><sup>5</sup></span> recently published a cross-sectional clinical study in <i>Diabetes</i> journal, examining the effect of metformin on DPN outcomes in patients with type 2 diabetes (Figure 1). The study involved 69 participants with type 2 diabetes receiving metformin therapy and 69 clinically matched participants who were not on metformin as part of standard clinical care. Participants not receiving metformin were prescribed other oral antihyperglycemic agents, such as SGLT2 inhibitors, DPP-4 inhibitors, and sulfonylureas. All participants underwent peripheral nerve ultrasonography of the median and tibial nerves to measure nerve cross-sectional area (CSA). Neurological assessments, including the modified Toronto Clinical Neuropathy Scale (mTCNS) and Total Neuropathy Score (TNS), were used to evaluate DPN severity, alongside nerve conduction studies performed on the tibial motor and sural sensory nerves. Peripheral nerve ultrasonography was indeed utilized in the study to assess the cross-sectional areas (CSA) of the tibial and median nerves.</p><p>In the metformin group, the mean duration of metformin therapy was 162 ± 14 months, with a mean daily dose of 1,523 ± 69 mg. Clinical assessments of peripheral neuropathy severity, as measured by mTCNS and TNS, revealed that the metformin group exhibited less severe neuropathic symptoms despite no significant differences in sural nerve amplitude or mean tibial compound muscle action potential. Supporting these findings, peripheral nerve ultrasonography demonstrated a significant reduction in the mean CSA of the median and tibial nerves in the metformin group compared to the nonmetformin group.</p><p>To further explore the mechanism, axonal excitability—which reflects the behavior of voltage-gated ion channels, particularly nodal Na+ and K+ channels—was analyzed. The metformin group showed lower mean stimulation for 50% of the maximal response and lower mean rheobase, both of which are proportional indicators of neuropathy severity. Additionally, the mean magnitude of subexcitability and S2 accommodation was higher in the metformin group, reflecting altered behavior of nodal slow K+ channels. Mathematical modeling of axonal excitability data in the non-metformin group suggested that changes in excitability values were best explained by reduced nodal Na+ permeability. Furthermore, when reduced Na+ permeability was combined with reduced slow K+ conductance in the model, it indicated less reduction in both nodal Na+ and slow K+ conductance in the metformin group compared to the non-metformin group. These findings suggest that metformin mitigates the reduction in axonal nodal Na+ permeability typically associated with DPN and promotes an increase in nodal slow K+ conductance, resulting in mild relative hyperpolarization of the neuronal membrane potential compared to the non-metformin group.</p><p>The most notable aspect of this study is the improvement in DPN severity attributed to metformin therapy. Indeed, experimental models of DPN have previously reported that metformin improves peripheral nerve function and pain perception. Metformin exerts a wide range of antidiabetic effects, including enhancing insulin sensitivity, inhibiting gluconeogenesis in the liver, countering glucagon effects, suppressing mitochondrial respiration, and activating 5' adenosine monophosphate-activated protein kinase. These effects likely contribute to the suppression of neuroinflammation and oxidative stress associated with DPN. Metformin has also been shown to improve ion channel localization and promote myelination in Schwann cells, findings that align with the observed improvements in Na+ and K+ channel function in this study.</p><p>In contrast, a prospective study involving clinically matched patients treated with metformin for 6 months reported that metformin worsened the severity of DPN, as evaluated by TCNS and nerve conduction studies, including median conduction velocity and sensory nerve action potentials of the superficial peroneal and sural nerves<span><sup>2</sup></span>. TCNS were significantly correlated with lower cobalamin levels and higher levels of methylmalonic acid and homocysteine. Multivariate analysis further identified metformin use as an independent negative prognostic factor. Additionally, prior studies have indicated a dose- and duration-dependent decrease in cobalamin and a corresponding worsening of neuropathy with metformin treatment<span><sup>2, 6</sup></span>.</p><p>In the present study, the mean daily metformin dose was 1,523 ± 69 mg, comparable to previous reports ranging from 1,000 to 2,000 mg<sup>2</sup>. The duration of metformin administration was over 10 years (162 ± 14 months), which is consistent with or longer than the administration periods described in other studies. Differences in dose and duration of metformin treatment are, therefore, unlikely to explain the variations in treatment outcomes. Moreover, patients in this study had relatively poorly controlled diabetes, with a mean disease duration of approximately 180 months and HbA1c levels exceeding 8%, in contrast to previous studies. These factors suggest that DPN improvement with metformin therapy would be less likely dependent on diabetes status in this study.</p><p>One plausible explanation for the discrepancy in metformin's effects on DPN lies in the use of more clinically and neuro-functionally matched cases in the current study. Although this study controlled the use of medications other than metformin, some of the previous reports lack information on other antidiabetic drugs. Consequently, differences in coadministered medications may account for the variability.</p><p>Another key difference is the evaluation methodology for DPN. Whereas most previous studies assessed DPN severity using TCNS, the present study employed mTCNS and TNS. The mTCNS omits tendon reflex evaluation, increasing sensitivity to early-stage DPN while maintaining high correlation with TCNS. Additionally, this study uniquely measured CSA of the median and tibial nerves using ultrasonography, revealing reduced nerve CSA with metformin. Prior studies demonstrated enlarged peripheral nerves in DPN via ultrasonography, attributing this to activation of the polyol pathway, osmotic changes, and intraneural edema. Further studies have also suggested Na+/K+ pump dysfunction and intracellular Na+ accumulation in diabetes as contributors to tibial nerve CSA enlargement in DPN. Supporting this, axonal excitability analysis—focused on voltage-gated nodal Na+ and K+ channels—identified reductions in nodal Na+ and slow K+ conductance.</p><p>These findings suggest that metformin can directly influence nerve ion channels of residual nerves in DPN, alleviating nerve severity despite the absence of electrophysiological improvement.</p><p>Discrepancies in previous study results may arise from differences in patient groups, the lack of CSA measurement via ultrasonography, or the absence of axonal excitability assessments. Nonetheless, several unanswered questions remain. Specifically, the correlation between cobalamin and its related metabolites, and CSA or axonal excitability requires further investigation, because cobalamin, homocysteine, and methylmalonic acid levels were not measured in this study. Furthermore, since the current study was cross-sectional, its findings must be validated through prospective, randomized trials. By addressing these limitations, metformin prescription for DPN may become more standardized and widely recommended in the future, with attention to monitoring cobalamin, homocysteine, and methylmalonic acid levels.</p><p>The author declares no conflict of interest.</p>","PeriodicalId":51250,"journal":{"name":"Journal of Diabetes Investigation","volume":"16 7","pages":"1151-1153"},"PeriodicalIF":3.0000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.70055","citationCount":"0","resultStr":"{\"title\":\"Questioning the pros and cons of metformin treatment in diabetic peripheral neuropathy\",\"authors\":\"Hiroki Mizukami\",\"doi\":\"10.1111/jdi.70055\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Diabetic peripheral neuropathy (DPN) is the most common complication among diabetic patients. Its symptoms include pain, hyperalgesia, hypoalgesia, and paralysis, all of which can significantly reduce patients' quality of life. In DPN, peripheral nerve fibers are affected as early as the prediabetic stage. Currently, no curative treatment has been established. As demonstrated in large clinical trials like the Diabetes Control and Complication Trial, strict glycemic control remains the only proven method to slow the progression of DPN. Consequently, it is crucial to identify which diabetes medications are more effective against neuropathy or, at the very least, do not exacerbate it.</p><p>Experimentally, various antidiabetic drugs—including dipeptidyl peptidase-4 (DPP-4) inhibitors, α-glucosidase inhibitors, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and incretin agonists—have shown therapeutic effects on DPN that are independent of blood glucose improvement<span><sup>1</sup></span>. Among oral antidiabetic agents, metformin is one of the most widely used drugs for diabetes. However, its effects on DPN remain controversial. Several studies have reported that metformin use decreases cobalamin (Vitamin B12) levels while increasing its related metabolite homocysteine and methylmalonic acid. Deficiency in cobalamin and elevated homocysteine and methylmalonic acid levels are known to induce peripheral neuropathy; hence, metformin has been suggested to worsen DPN<span><sup>2</sup></span>. On the other hand, some studies indicate that metformin has no apparent effect on DPN<span><sup>3</sup></span>. Furthermore, other research suggests that while metformin reduces cobalamin levels, it does not influence DPN progression<span><sup>4</sup></span>. As such, the therapeutic effects of metformin on DPN remain contentious.</p><p>In this context, Dhanapalaratnam <i>et al</i>.<span><sup>5</sup></span> recently published a cross-sectional clinical study in <i>Diabetes</i> journal, examining the effect of metformin on DPN outcomes in patients with type 2 diabetes (Figure 1). The study involved 69 participants with type 2 diabetes receiving metformin therapy and 69 clinically matched participants who were not on metformin as part of standard clinical care. Participants not receiving metformin were prescribed other oral antihyperglycemic agents, such as SGLT2 inhibitors, DPP-4 inhibitors, and sulfonylureas. All participants underwent peripheral nerve ultrasonography of the median and tibial nerves to measure nerve cross-sectional area (CSA). Neurological assessments, including the modified Toronto Clinical Neuropathy Scale (mTCNS) and Total Neuropathy Score (TNS), were used to evaluate DPN severity, alongside nerve conduction studies performed on the tibial motor and sural sensory nerves. Peripheral nerve ultrasonography was indeed utilized in the study to assess the cross-sectional areas (CSA) of the tibial and median nerves.</p><p>In the metformin group, the mean duration of metformin therapy was 162 ± 14 months, with a mean daily dose of 1,523 ± 69 mg. Clinical assessments of peripheral neuropathy severity, as measured by mTCNS and TNS, revealed that the metformin group exhibited less severe neuropathic symptoms despite no significant differences in sural nerve amplitude or mean tibial compound muscle action potential. Supporting these findings, peripheral nerve ultrasonography demonstrated a significant reduction in the mean CSA of the median and tibial nerves in the metformin group compared to the nonmetformin group.</p><p>To further explore the mechanism, axonal excitability—which reflects the behavior of voltage-gated ion channels, particularly nodal Na+ and K+ channels—was analyzed. The metformin group showed lower mean stimulation for 50% of the maximal response and lower mean rheobase, both of which are proportional indicators of neuropathy severity. Additionally, the mean magnitude of subexcitability and S2 accommodation was higher in the metformin group, reflecting altered behavior of nodal slow K+ channels. Mathematical modeling of axonal excitability data in the non-metformin group suggested that changes in excitability values were best explained by reduced nodal Na+ permeability. Furthermore, when reduced Na+ permeability was combined with reduced slow K+ conductance in the model, it indicated less reduction in both nodal Na+ and slow K+ conductance in the metformin group compared to the non-metformin group. These findings suggest that metformin mitigates the reduction in axonal nodal Na+ permeability typically associated with DPN and promotes an increase in nodal slow K+ conductance, resulting in mild relative hyperpolarization of the neuronal membrane potential compared to the non-metformin group.</p><p>The most notable aspect of this study is the improvement in DPN severity attributed to metformin therapy. Indeed, experimental models of DPN have previously reported that metformin improves peripheral nerve function and pain perception. Metformin exerts a wide range of antidiabetic effects, including enhancing insulin sensitivity, inhibiting gluconeogenesis in the liver, countering glucagon effects, suppressing mitochondrial respiration, and activating 5' adenosine monophosphate-activated protein kinase. These effects likely contribute to the suppression of neuroinflammation and oxidative stress associated with DPN. Metformin has also been shown to improve ion channel localization and promote myelination in Schwann cells, findings that align with the observed improvements in Na+ and K+ channel function in this study.</p><p>In contrast, a prospective study involving clinically matched patients treated with metformin for 6 months reported that metformin worsened the severity of DPN, as evaluated by TCNS and nerve conduction studies, including median conduction velocity and sensory nerve action potentials of the superficial peroneal and sural nerves<span><sup>2</sup></span>. TCNS were significantly correlated with lower cobalamin levels and higher levels of methylmalonic acid and homocysteine. Multivariate analysis further identified metformin use as an independent negative prognostic factor. Additionally, prior studies have indicated a dose- and duration-dependent decrease in cobalamin and a corresponding worsening of neuropathy with metformin treatment<span><sup>2, 6</sup></span>.</p><p>In the present study, the mean daily metformin dose was 1,523 ± 69 mg, comparable to previous reports ranging from 1,000 to 2,000 mg<sup>2</sup>. The duration of metformin administration was over 10 years (162 ± 14 months), which is consistent with or longer than the administration periods described in other studies. Differences in dose and duration of metformin treatment are, therefore, unlikely to explain the variations in treatment outcomes. Moreover, patients in this study had relatively poorly controlled diabetes, with a mean disease duration of approximately 180 months and HbA1c levels exceeding 8%, in contrast to previous studies. These factors suggest that DPN improvement with metformin therapy would be less likely dependent on diabetes status in this study.</p><p>One plausible explanation for the discrepancy in metformin's effects on DPN lies in the use of more clinically and neuro-functionally matched cases in the current study. Although this study controlled the use of medications other than metformin, some of the previous reports lack information on other antidiabetic drugs. Consequently, differences in coadministered medications may account for the variability.</p><p>Another key difference is the evaluation methodology for DPN. Whereas most previous studies assessed DPN severity using TCNS, the present study employed mTCNS and TNS. The mTCNS omits tendon reflex evaluation, increasing sensitivity to early-stage DPN while maintaining high correlation with TCNS. Additionally, this study uniquely measured CSA of the median and tibial nerves using ultrasonography, revealing reduced nerve CSA with metformin. Prior studies demonstrated enlarged peripheral nerves in DPN via ultrasonography, attributing this to activation of the polyol pathway, osmotic changes, and intraneural edema. Further studies have also suggested Na+/K+ pump dysfunction and intracellular Na+ accumulation in diabetes as contributors to tibial nerve CSA enlargement in DPN. Supporting this, axonal excitability analysis—focused on voltage-gated nodal Na+ and K+ channels—identified reductions in nodal Na+ and slow K+ conductance.</p><p>These findings suggest that metformin can directly influence nerve ion channels of residual nerves in DPN, alleviating nerve severity despite the absence of electrophysiological improvement.</p><p>Discrepancies in previous study results may arise from differences in patient groups, the lack of CSA measurement via ultrasonography, or the absence of axonal excitability assessments. Nonetheless, several unanswered questions remain. Specifically, the correlation between cobalamin and its related metabolites, and CSA or axonal excitability requires further investigation, because cobalamin, homocysteine, and methylmalonic acid levels were not measured in this study. Furthermore, since the current study was cross-sectional, its findings must be validated through prospective, randomized trials. By addressing these limitations, metformin prescription for DPN may become more standardized and widely recommended in the future, with attention to monitoring cobalamin, homocysteine, and methylmalonic acid levels.</p><p>The author declares no conflict of interest.</p>\",\"PeriodicalId\":51250,\"journal\":{\"name\":\"Journal of Diabetes Investigation\",\"volume\":\"16 7\",\"pages\":\"1151-1153\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.70055\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Diabetes Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jdi.70055\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Diabetes Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jdi.70055","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Questioning the pros and cons of metformin treatment in diabetic peripheral neuropathy
Diabetic peripheral neuropathy (DPN) is the most common complication among diabetic patients. Its symptoms include pain, hyperalgesia, hypoalgesia, and paralysis, all of which can significantly reduce patients' quality of life. In DPN, peripheral nerve fibers are affected as early as the prediabetic stage. Currently, no curative treatment has been established. As demonstrated in large clinical trials like the Diabetes Control and Complication Trial, strict glycemic control remains the only proven method to slow the progression of DPN. Consequently, it is crucial to identify which diabetes medications are more effective against neuropathy or, at the very least, do not exacerbate it.
Experimentally, various antidiabetic drugs—including dipeptidyl peptidase-4 (DPP-4) inhibitors, α-glucosidase inhibitors, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and incretin agonists—have shown therapeutic effects on DPN that are independent of blood glucose improvement1. Among oral antidiabetic agents, metformin is one of the most widely used drugs for diabetes. However, its effects on DPN remain controversial. Several studies have reported that metformin use decreases cobalamin (Vitamin B12) levels while increasing its related metabolite homocysteine and methylmalonic acid. Deficiency in cobalamin and elevated homocysteine and methylmalonic acid levels are known to induce peripheral neuropathy; hence, metformin has been suggested to worsen DPN2. On the other hand, some studies indicate that metformin has no apparent effect on DPN3. Furthermore, other research suggests that while metformin reduces cobalamin levels, it does not influence DPN progression4. As such, the therapeutic effects of metformin on DPN remain contentious.
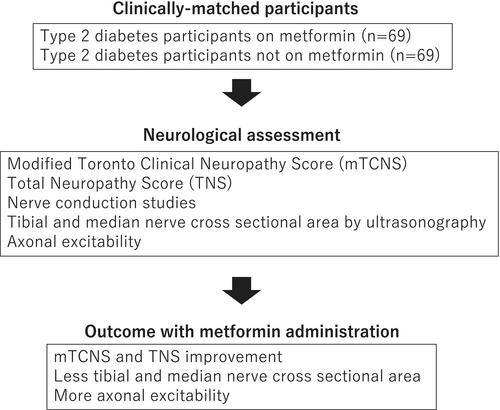
In this context, Dhanapalaratnam et al.5 recently published a cross-sectional clinical study in Diabetes journal, examining the effect of metformin on DPN outcomes in patients with type 2 diabetes (Figure 1). The study involved 69 participants with type 2 diabetes receiving metformin therapy and 69 clinically matched participants who were not on metformin as part of standard clinical care. Participants not receiving metformin were prescribed other oral antihyperglycemic agents, such as SGLT2 inhibitors, DPP-4 inhibitors, and sulfonylureas. All participants underwent peripheral nerve ultrasonography of the median and tibial nerves to measure nerve cross-sectional area (CSA). Neurological assessments, including the modified Toronto Clinical Neuropathy Scale (mTCNS) and Total Neuropathy Score (TNS), were used to evaluate DPN severity, alongside nerve conduction studies performed on the tibial motor and sural sensory nerves. Peripheral nerve ultrasonography was indeed utilized in the study to assess the cross-sectional areas (CSA) of the tibial and median nerves.
In the metformin group, the mean duration of metformin therapy was 162 ± 14 months, with a mean daily dose of 1,523 ± 69 mg. Clinical assessments of peripheral neuropathy severity, as measured by mTCNS and TNS, revealed that the metformin group exhibited less severe neuropathic symptoms despite no significant differences in sural nerve amplitude or mean tibial compound muscle action potential. Supporting these findings, peripheral nerve ultrasonography demonstrated a significant reduction in the mean CSA of the median and tibial nerves in the metformin group compared to the nonmetformin group.
To further explore the mechanism, axonal excitability—which reflects the behavior of voltage-gated ion channels, particularly nodal Na+ and K+ channels—was analyzed. The metformin group showed lower mean stimulation for 50% of the maximal response and lower mean rheobase, both of which are proportional indicators of neuropathy severity. Additionally, the mean magnitude of subexcitability and S2 accommodation was higher in the metformin group, reflecting altered behavior of nodal slow K+ channels. Mathematical modeling of axonal excitability data in the non-metformin group suggested that changes in excitability values were best explained by reduced nodal Na+ permeability. Furthermore, when reduced Na+ permeability was combined with reduced slow K+ conductance in the model, it indicated less reduction in both nodal Na+ and slow K+ conductance in the metformin group compared to the non-metformin group. These findings suggest that metformin mitigates the reduction in axonal nodal Na+ permeability typically associated with DPN and promotes an increase in nodal slow K+ conductance, resulting in mild relative hyperpolarization of the neuronal membrane potential compared to the non-metformin group.
The most notable aspect of this study is the improvement in DPN severity attributed to metformin therapy. Indeed, experimental models of DPN have previously reported that metformin improves peripheral nerve function and pain perception. Metformin exerts a wide range of antidiabetic effects, including enhancing insulin sensitivity, inhibiting gluconeogenesis in the liver, countering glucagon effects, suppressing mitochondrial respiration, and activating 5' adenosine monophosphate-activated protein kinase. These effects likely contribute to the suppression of neuroinflammation and oxidative stress associated with DPN. Metformin has also been shown to improve ion channel localization and promote myelination in Schwann cells, findings that align with the observed improvements in Na+ and K+ channel function in this study.
In contrast, a prospective study involving clinically matched patients treated with metformin for 6 months reported that metformin worsened the severity of DPN, as evaluated by TCNS and nerve conduction studies, including median conduction velocity and sensory nerve action potentials of the superficial peroneal and sural nerves2. TCNS were significantly correlated with lower cobalamin levels and higher levels of methylmalonic acid and homocysteine. Multivariate analysis further identified metformin use as an independent negative prognostic factor. Additionally, prior studies have indicated a dose- and duration-dependent decrease in cobalamin and a corresponding worsening of neuropathy with metformin treatment2, 6.
In the present study, the mean daily metformin dose was 1,523 ± 69 mg, comparable to previous reports ranging from 1,000 to 2,000 mg2. The duration of metformin administration was over 10 years (162 ± 14 months), which is consistent with or longer than the administration periods described in other studies. Differences in dose and duration of metformin treatment are, therefore, unlikely to explain the variations in treatment outcomes. Moreover, patients in this study had relatively poorly controlled diabetes, with a mean disease duration of approximately 180 months and HbA1c levels exceeding 8%, in contrast to previous studies. These factors suggest that DPN improvement with metformin therapy would be less likely dependent on diabetes status in this study.
One plausible explanation for the discrepancy in metformin's effects on DPN lies in the use of more clinically and neuro-functionally matched cases in the current study. Although this study controlled the use of medications other than metformin, some of the previous reports lack information on other antidiabetic drugs. Consequently, differences in coadministered medications may account for the variability.
Another key difference is the evaluation methodology for DPN. Whereas most previous studies assessed DPN severity using TCNS, the present study employed mTCNS and TNS. The mTCNS omits tendon reflex evaluation, increasing sensitivity to early-stage DPN while maintaining high correlation with TCNS. Additionally, this study uniquely measured CSA of the median and tibial nerves using ultrasonography, revealing reduced nerve CSA with metformin. Prior studies demonstrated enlarged peripheral nerves in DPN via ultrasonography, attributing this to activation of the polyol pathway, osmotic changes, and intraneural edema. Further studies have also suggested Na+/K+ pump dysfunction and intracellular Na+ accumulation in diabetes as contributors to tibial nerve CSA enlargement in DPN. Supporting this, axonal excitability analysis—focused on voltage-gated nodal Na+ and K+ channels—identified reductions in nodal Na+ and slow K+ conductance.
These findings suggest that metformin can directly influence nerve ion channels of residual nerves in DPN, alleviating nerve severity despite the absence of electrophysiological improvement.
Discrepancies in previous study results may arise from differences in patient groups, the lack of CSA measurement via ultrasonography, or the absence of axonal excitability assessments. Nonetheless, several unanswered questions remain. Specifically, the correlation between cobalamin and its related metabolites, and CSA or axonal excitability requires further investigation, because cobalamin, homocysteine, and methylmalonic acid levels were not measured in this study. Furthermore, since the current study was cross-sectional, its findings must be validated through prospective, randomized trials. By addressing these limitations, metformin prescription for DPN may become more standardized and widely recommended in the future, with attention to monitoring cobalamin, homocysteine, and methylmalonic acid levels.
期刊介绍:
Journal of Diabetes Investigation is your core diabetes journal from Asia; the official journal of the Asian Association for the Study of Diabetes (AASD). The journal publishes original research, country reports, commentaries, reviews, mini-reviews, case reports, letters, as well as editorials and news. Embracing clinical and experimental research in diabetes and related areas, the Journal of Diabetes Investigation includes aspects of prevention, treatment, as well as molecular aspects and pathophysiology. Translational research focused on the exchange of ideas between clinicians and researchers is also welcome. Journal of Diabetes Investigation is indexed by Science Citation Index Expanded (SCIE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


