Jonas Brinck, Karin Littmann, Daniel Eriksson Hogling, Linnea Widman, Kenneth Caidahl, Maria Eriksson, Jonas Johnson, Karolina Szummer, Magnus Bäck
{"title":"多普勒超声心动图测量的脂蛋白升高(a)和主动脉狭窄进展:一项基于人群的队列研究。","authors":"Jonas Brinck, Karin Littmann, Daniel Eriksson Hogling, Linnea Widman, Kenneth Caidahl, Maria Eriksson, Jonas Johnson, Karolina Szummer, Magnus Bäck","doi":"10.1111/joim.20095","DOIUrl":null,"url":null,"abstract":"<p>Elevated lipoprotein(a) (Lp(a)) is a dyslipoproteinaemia that causes atherosclerotic cardiovascular disease and calcified aortic valve stenosis (AS) [<span>1, 2</span>]. AS develops over decades and can lead to valve obstruction requiring an aortic valve procedure. Both genetic variations in the LPA gene and an elevated plasma Lp(a) level are associated with an increased incidence of AS [<span>3, 4</span>]. Measurement of peak aortic jet velocity (<i>V</i><sub>max</sub>; m/s) with Doppler echocardiography is used to assess and monitor AS in clinical routine. In the ASTRONOMER trial, a limited number of participants (<i>n</i> = 220) with mild-to-moderate AS (initial <i>V</i><sub>max</sub> ≥ 2.5 m/s) who underwent repeated echocardiography exhibited faster <i>V</i><sub>max</sub> progression with elevated Lp(a) [<span>5-7</span>]. Similar faster haemodynamic progression at higher Lp(a) levels was reported in 129 subjects with AS (initial <i>V</i><sub>max</sub> ≥ 2.0 m/s) from the SATIRE trial and Ring of Fire study [<span>8</span>]. However, the impact of Lp(a) on AS progression in an unselected population has remained unexplored. The aim of the present study was to determine the effect of elevated plasma Lp(a) on AS progression measured as <i>V</i><sub>max</sub> by repeated Doppler echocardiography in a large cohort with and without AS at any stage.</p><p>We performed an observational retrospective cohort study by linking two databases of individuals who had had their plasma Lp(a) level measured 2003–2017 (<i>n</i> = 23,398) and who had ≥2 Doppler echocardiography <i>V</i><sub>max</sub> measurements with ≥6 months of interval 2003–2018 (<i>n</i> = 9889) in the clinical routine in Region Stockholm, Sweden (Fig. S1). Lp(a) was analysed using accredited laboratory methods, reporting values in nmol/L or mg/dL as previously described [<span>9</span>]. Participants were subdivided into three Lp(a) strata defined as low (<70 nmol/L or <30 mg/dL), intermediate (70–169 nmol/L or 30–69 mg/dL) and high (≥170 nmol/L or ≥70 mg/dL). Transthoracic Doppler echocardiography was performed at Karolinska University Hospital using standard equipment. The current European Society of Cardiology guidelines recommendation on AS management in relation to AS progression is based on the change in <i>V</i><sub>max</sub>, measured in m/s/year, which was calculated in the present study as the difference between the first and the last Doppler measurement divided by the time interval. Individuals who underwent aortic valve replacement (AVR) were excluded if the procedure was performed before the first echocardiography and censored if undergoing AVR during the observational period. The individuals’ cardiovascular status was specified by the International Classification of Diseases diagnoses. Differences between individuals in Lp(a) strata were compared using the Kruskal–Wallis test, Dunn's post hoc test and unbalanced adjusted analysis of covariance with ranked transformed data. The study was approved by the Ethical Review Authority.</p><p>A total of 694 subjects (average 3.5 Doppler measurements/subject) met the study criteria and were allocated to the low (<i>n</i> = 434), intermediate (<i>n</i> = 125) and high (<i>n</i> = 135) Lp(a) subgroups (Table S1). The mean age in the groups was 51, 50 and 58 years, and the proportion of women was 37%, 43% and 39%, respectively, at the timepoint of the first Doppler measurement. The initial median <i>V</i><sub>max</sub> and the median follow-up time of <i>V</i><sub>max</sub> progression were similar between subgroups with 1.42 m/s and 3.7 years (low), 1.44 m/s and 2.9 years (intermediate), and 1.42 m/s and 3.0 years (high) (<i>p</i> = 0.82 and 0.35). The median (25th–75th percentile) progression rates were 0.01 (−0.04 to 0.07), 0.02 (−0.03 to 0.14) and 0.03 (−0.02 to 0.12) m/s/year, respectively (<i>p</i> = 0.013) (Fig. 1). The difference in <i>V</i><sub>max</sub> progression between Lp(a) strata remained significant after adjustment for age, sex and baseline <i>V</i><sub>max</sub> (<i>p</i> = 0.027). The <i>V</i><sub>max</sub> progression was significantly higher in the intermediate (<i>p</i> = 0.039) and high (<i>p</i> = 0.003) compared with the reference low Lp(a) subgroups. When including only individuals with an initial <i>V</i><sub>max</sub> of >1.5 m/s, the median rates increased in the high Lp(a) group to 0.05 (−0.04 to 0.20) m/s/year compared to neutral median rates of 0.00 (−0.10 to 0.11) m/s/year in the corresponding low Lp(a) group and 0.00 (−0.04 to 0.13) m/s/year in the intermediate Lp(a) group (<i>p</i> = 0.058). As a reference, individuals with ≥2 Doppler measurements but without a Lp(a) measurement (<i>n</i> = 9195) had no change in annual median <i>V</i><sub>max</sub> (0.00 [−0.07 to 0.08] m/s/year) during a median follow-up of 3.0 years (Fig. 1).</p><p>This is the first report associating high plasma Lp(a) with a 3-fold faster <i>V</i><sub>max</sub> progression compared to low Lp(a) in the general population regardless of the presence or absence of AS at any stage at baseline. Although the <i>V</i><sub>max</sub> progression was low compared to individuals with mild-to-moderate AS [<span>5, 8</span>], the <i>V</i><sub>max</sub> progression rates are not linear with time. An early small increase in <i>V</i><sub>max</sub> progression will shorten the time to stages of accelerated <i>V</i><sub>max</sub> progression towards AS. The present study highlights the long-term effects of Lp(a) exposure for AS development and identifies Lp(a) as a potential biomarker of AS progression in the general population. These results identify high Lp(a) as a possible indicator of the need for echocardiographic surveillance of AS development. The clinical implications are, however, limited by the fact that, at present, no therapy exists to slow down AS progression [<span>10</span>].</p><p><b>Jonas Brinck</b>, <b>Karin Littmann</b> and <b>Magnus Bäck</b>: Conceptualization; visualization; investigation; writing; editing and reviewing. <b>Jonas Brinck</b> and <b>Magnus Bäck</b>: Project administration and funding acquisition. <b>Linnea Widman</b>: Methodology/Statistics; reviewing. <b>Daniel Eriksson Hogling</b>, <b>Kenneth Caidahl</b>, <b>Maria Eriksson</b> and <b>Karolina Szummer</b>: Reviewing; editing. All authors approve the final version for publication and agree to be accountable for all aspects of the work.</p><p>JB reports institutional grants from Amgen, Novartis and Ionis outside the submitted work, and honoraria from Amgen, Novartis, Sanofi and Ultragenyx. DEH has received institutional honoraria from Amgen. KL reports research grant funding from Amgen and Stockholm Innovation Fund outside the submitted work and honoraria from Amgen and Sanofi. MBs’ institution has received speaker and consultant fees from Amarin, Amgen, Heel, Novartis and Fresenius Kabi. The remaining authors have nothing to disclose in relation to this work.</p><p>MB is supported by the Swedish Research Council, Grant Number: 2023-02652; Heart-Lung Foundation, Grant Number: 20240697.</p><p>The study was approved by the Ethical Review Authority.</p>","PeriodicalId":196,"journal":{"name":"Journal of Internal Medicine","volume":"298 1","pages":"46-48"},"PeriodicalIF":9.2000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.20095","citationCount":"0","resultStr":"{\"title\":\"Elevated lipoprotein(a) and progression of aortic stenosis measured by Doppler echocardiography: A population-based cohort study\",\"authors\":\"Jonas Brinck, Karin Littmann, Daniel Eriksson Hogling, Linnea Widman, Kenneth Caidahl, Maria Eriksson, Jonas Johnson, Karolina Szummer, Magnus Bäck\",\"doi\":\"10.1111/joim.20095\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Elevated lipoprotein(a) (Lp(a)) is a dyslipoproteinaemia that causes atherosclerotic cardiovascular disease and calcified aortic valve stenosis (AS) [<span>1, 2</span>]. AS develops over decades and can lead to valve obstruction requiring an aortic valve procedure. Both genetic variations in the LPA gene and an elevated plasma Lp(a) level are associated with an increased incidence of AS [<span>3, 4</span>]. Measurement of peak aortic jet velocity (<i>V</i><sub>max</sub>; m/s) with Doppler echocardiography is used to assess and monitor AS in clinical routine. In the ASTRONOMER trial, a limited number of participants (<i>n</i> = 220) with mild-to-moderate AS (initial <i>V</i><sub>max</sub> ≥ 2.5 m/s) who underwent repeated echocardiography exhibited faster <i>V</i><sub>max</sub> progression with elevated Lp(a) [<span>5-7</span>]. Similar faster haemodynamic progression at higher Lp(a) levels was reported in 129 subjects with AS (initial <i>V</i><sub>max</sub> ≥ 2.0 m/s) from the SATIRE trial and Ring of Fire study [<span>8</span>]. However, the impact of Lp(a) on AS progression in an unselected population has remained unexplored. The aim of the present study was to determine the effect of elevated plasma Lp(a) on AS progression measured as <i>V</i><sub>max</sub> by repeated Doppler echocardiography in a large cohort with and without AS at any stage.</p><p>We performed an observational retrospective cohort study by linking two databases of individuals who had had their plasma Lp(a) level measured 2003–2017 (<i>n</i> = 23,398) and who had ≥2 Doppler echocardiography <i>V</i><sub>max</sub> measurements with ≥6 months of interval 2003–2018 (<i>n</i> = 9889) in the clinical routine in Region Stockholm, Sweden (Fig. S1). Lp(a) was analysed using accredited laboratory methods, reporting values in nmol/L or mg/dL as previously described [<span>9</span>]. Participants were subdivided into three Lp(a) strata defined as low (<70 nmol/L or <30 mg/dL), intermediate (70–169 nmol/L or 30–69 mg/dL) and high (≥170 nmol/L or ≥70 mg/dL). Transthoracic Doppler echocardiography was performed at Karolinska University Hospital using standard equipment. The current European Society of Cardiology guidelines recommendation on AS management in relation to AS progression is based on the change in <i>V</i><sub>max</sub>, measured in m/s/year, which was calculated in the present study as the difference between the first and the last Doppler measurement divided by the time interval. Individuals who underwent aortic valve replacement (AVR) were excluded if the procedure was performed before the first echocardiography and censored if undergoing AVR during the observational period. The individuals’ cardiovascular status was specified by the International Classification of Diseases diagnoses. Differences between individuals in Lp(a) strata were compared using the Kruskal–Wallis test, Dunn's post hoc test and unbalanced adjusted analysis of covariance with ranked transformed data. The study was approved by the Ethical Review Authority.</p><p>A total of 694 subjects (average 3.5 Doppler measurements/subject) met the study criteria and were allocated to the low (<i>n</i> = 434), intermediate (<i>n</i> = 125) and high (<i>n</i> = 135) Lp(a) subgroups (Table S1). The mean age in the groups was 51, 50 and 58 years, and the proportion of women was 37%, 43% and 39%, respectively, at the timepoint of the first Doppler measurement. The initial median <i>V</i><sub>max</sub> and the median follow-up time of <i>V</i><sub>max</sub> progression were similar between subgroups with 1.42 m/s and 3.7 years (low), 1.44 m/s and 2.9 years (intermediate), and 1.42 m/s and 3.0 years (high) (<i>p</i> = 0.82 and 0.35). The median (25th–75th percentile) progression rates were 0.01 (−0.04 to 0.07), 0.02 (−0.03 to 0.14) and 0.03 (−0.02 to 0.12) m/s/year, respectively (<i>p</i> = 0.013) (Fig. 1). The difference in <i>V</i><sub>max</sub> progression between Lp(a) strata remained significant after adjustment for age, sex and baseline <i>V</i><sub>max</sub> (<i>p</i> = 0.027). The <i>V</i><sub>max</sub> progression was significantly higher in the intermediate (<i>p</i> = 0.039) and high (<i>p</i> = 0.003) compared with the reference low Lp(a) subgroups. When including only individuals with an initial <i>V</i><sub>max</sub> of >1.5 m/s, the median rates increased in the high Lp(a) group to 0.05 (−0.04 to 0.20) m/s/year compared to neutral median rates of 0.00 (−0.10 to 0.11) m/s/year in the corresponding low Lp(a) group and 0.00 (−0.04 to 0.13) m/s/year in the intermediate Lp(a) group (<i>p</i> = 0.058). As a reference, individuals with ≥2 Doppler measurements but without a Lp(a) measurement (<i>n</i> = 9195) had no change in annual median <i>V</i><sub>max</sub> (0.00 [−0.07 to 0.08] m/s/year) during a median follow-up of 3.0 years (Fig. 1).</p><p>This is the first report associating high plasma Lp(a) with a 3-fold faster <i>V</i><sub>max</sub> progression compared to low Lp(a) in the general population regardless of the presence or absence of AS at any stage at baseline. Although the <i>V</i><sub>max</sub> progression was low compared to individuals with mild-to-moderate AS [<span>5, 8</span>], the <i>V</i><sub>max</sub> progression rates are not linear with time. An early small increase in <i>V</i><sub>max</sub> progression will shorten the time to stages of accelerated <i>V</i><sub>max</sub> progression towards AS. The present study highlights the long-term effects of Lp(a) exposure for AS development and identifies Lp(a) as a potential biomarker of AS progression in the general population. These results identify high Lp(a) as a possible indicator of the need for echocardiographic surveillance of AS development. The clinical implications are, however, limited by the fact that, at present, no therapy exists to slow down AS progression [<span>10</span>].</p><p><b>Jonas Brinck</b>, <b>Karin Littmann</b> and <b>Magnus Bäck</b>: Conceptualization; visualization; investigation; writing; editing and reviewing. <b>Jonas Brinck</b> and <b>Magnus Bäck</b>: Project administration and funding acquisition. <b>Linnea Widman</b>: Methodology/Statistics; reviewing. <b>Daniel Eriksson Hogling</b>, <b>Kenneth Caidahl</b>, <b>Maria Eriksson</b> and <b>Karolina Szummer</b>: Reviewing; editing. All authors approve the final version for publication and agree to be accountable for all aspects of the work.</p><p>JB reports institutional grants from Amgen, Novartis and Ionis outside the submitted work, and honoraria from Amgen, Novartis, Sanofi and Ultragenyx. DEH has received institutional honoraria from Amgen. KL reports research grant funding from Amgen and Stockholm Innovation Fund outside the submitted work and honoraria from Amgen and Sanofi. MBs’ institution has received speaker and consultant fees from Amarin, Amgen, Heel, Novartis and Fresenius Kabi. The remaining authors have nothing to disclose in relation to this work.</p><p>MB is supported by the Swedish Research Council, Grant Number: 2023-02652; Heart-Lung Foundation, Grant Number: 20240697.</p><p>The study was approved by the Ethical Review Authority.</p>\",\"PeriodicalId\":196,\"journal\":{\"name\":\"Journal of Internal Medicine\",\"volume\":\"298 1\",\"pages\":\"46-48\"},\"PeriodicalIF\":9.2000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.20095\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Internal Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/joim.20095\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/joim.20095","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
本研究强调了Lp(a)暴露对AS发展的长期影响,并确定Lp(a)是一般人群中AS进展的潜在生物标志物。这些结果确定高Lp(a)可能是需要超声心动图监测as发展的一个指标。然而,临床意义受到限制,因为目前还没有治疗方法可以减缓AS的进展。Jonas Brinck, Karin Littmann和Magnus Bäck:概念化;可视化;调查;写作;编辑和审查。Jonas Brinck和Magnus Bäck:项目管理和资金获取。Linnea Widman:方法论/统计;回顾。丹尼尔·埃里克森·霍格林,肯尼斯·凯达尔,玛丽亚·埃里克森和卡罗琳娜·夏莫:回顾;编辑。所有作者同意出版最终版本,并同意对工作的各个方面负责。JB报告了安进、诺华和Ionis在提交工作之外的机构资助,以及安进、诺华、赛诺菲和Ultragenyx的酬金。DEH获得了安进的机构荣誉。在提交的工作和安进和赛诺菲的酬金之外,KL报告了来自安进和斯德哥尔摩创新基金的研究资助资金。MBs的机构已经从Amarin、安进(Amgen)、Heel、诺华(Novartis)和费森尤斯卡比(Fresenius Kabi)获得了演讲和咨询费。其余的作者对这项工作没有什么可透露的。MB由瑞典研究委员会资助,资助号:2023-02652;心肺基金会,资助号:20240697。这项研究得到了伦理审查机构的批准。
Elevated lipoprotein(a) and progression of aortic stenosis measured by Doppler echocardiography: A population-based cohort study
Elevated lipoprotein(a) (Lp(a)) is a dyslipoproteinaemia that causes atherosclerotic cardiovascular disease and calcified aortic valve stenosis (AS) [1, 2]. AS develops over decades and can lead to valve obstruction requiring an aortic valve procedure. Both genetic variations in the LPA gene and an elevated plasma Lp(a) level are associated with an increased incidence of AS [3, 4]. Measurement of peak aortic jet velocity (Vmax; m/s) with Doppler echocardiography is used to assess and monitor AS in clinical routine. In the ASTRONOMER trial, a limited number of participants (n = 220) with mild-to-moderate AS (initial Vmax ≥ 2.5 m/s) who underwent repeated echocardiography exhibited faster Vmax progression with elevated Lp(a) [5-7]. Similar faster haemodynamic progression at higher Lp(a) levels was reported in 129 subjects with AS (initial Vmax ≥ 2.0 m/s) from the SATIRE trial and Ring of Fire study [8]. However, the impact of Lp(a) on AS progression in an unselected population has remained unexplored. The aim of the present study was to determine the effect of elevated plasma Lp(a) on AS progression measured as Vmax by repeated Doppler echocardiography in a large cohort with and without AS at any stage.
We performed an observational retrospective cohort study by linking two databases of individuals who had had their plasma Lp(a) level measured 2003–2017 (n = 23,398) and who had ≥2 Doppler echocardiography Vmax measurements with ≥6 months of interval 2003–2018 (n = 9889) in the clinical routine in Region Stockholm, Sweden (Fig. S1). Lp(a) was analysed using accredited laboratory methods, reporting values in nmol/L or mg/dL as previously described [9]. Participants were subdivided into three Lp(a) strata defined as low (<70 nmol/L or <30 mg/dL), intermediate (70–169 nmol/L or 30–69 mg/dL) and high (≥170 nmol/L or ≥70 mg/dL). Transthoracic Doppler echocardiography was performed at Karolinska University Hospital using standard equipment. The current European Society of Cardiology guidelines recommendation on AS management in relation to AS progression is based on the change in Vmax, measured in m/s/year, which was calculated in the present study as the difference between the first and the last Doppler measurement divided by the time interval. Individuals who underwent aortic valve replacement (AVR) were excluded if the procedure was performed before the first echocardiography and censored if undergoing AVR during the observational period. The individuals’ cardiovascular status was specified by the International Classification of Diseases diagnoses. Differences between individuals in Lp(a) strata were compared using the Kruskal–Wallis test, Dunn's post hoc test and unbalanced adjusted analysis of covariance with ranked transformed data. The study was approved by the Ethical Review Authority.
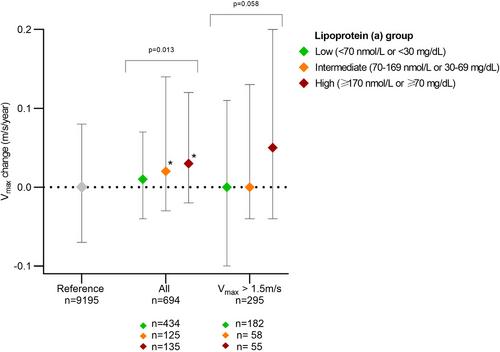
A total of 694 subjects (average 3.5 Doppler measurements/subject) met the study criteria and were allocated to the low (n = 434), intermediate (n = 125) and high (n = 135) Lp(a) subgroups (Table S1). The mean age in the groups was 51, 50 and 58 years, and the proportion of women was 37%, 43% and 39%, respectively, at the timepoint of the first Doppler measurement. The initial median Vmax and the median follow-up time of Vmax progression were similar between subgroups with 1.42 m/s and 3.7 years (low), 1.44 m/s and 2.9 years (intermediate), and 1.42 m/s and 3.0 years (high) (p = 0.82 and 0.35). The median (25th–75th percentile) progression rates were 0.01 (−0.04 to 0.07), 0.02 (−0.03 to 0.14) and 0.03 (−0.02 to 0.12) m/s/year, respectively (p = 0.013) (Fig. 1). The difference in Vmax progression between Lp(a) strata remained significant after adjustment for age, sex and baseline Vmax (p = 0.027). The Vmax progression was significantly higher in the intermediate (p = 0.039) and high (p = 0.003) compared with the reference low Lp(a) subgroups. When including only individuals with an initial Vmax of >1.5 m/s, the median rates increased in the high Lp(a) group to 0.05 (−0.04 to 0.20) m/s/year compared to neutral median rates of 0.00 (−0.10 to 0.11) m/s/year in the corresponding low Lp(a) group and 0.00 (−0.04 to 0.13) m/s/year in the intermediate Lp(a) group (p = 0.058). As a reference, individuals with ≥2 Doppler measurements but without a Lp(a) measurement (n = 9195) had no change in annual median Vmax (0.00 [−0.07 to 0.08] m/s/year) during a median follow-up of 3.0 years (Fig. 1).
This is the first report associating high plasma Lp(a) with a 3-fold faster Vmax progression compared to low Lp(a) in the general population regardless of the presence or absence of AS at any stage at baseline. Although the Vmax progression was low compared to individuals with mild-to-moderate AS [5, 8], the Vmax progression rates are not linear with time. An early small increase in Vmax progression will shorten the time to stages of accelerated Vmax progression towards AS. The present study highlights the long-term effects of Lp(a) exposure for AS development and identifies Lp(a) as a potential biomarker of AS progression in the general population. These results identify high Lp(a) as a possible indicator of the need for echocardiographic surveillance of AS development. The clinical implications are, however, limited by the fact that, at present, no therapy exists to slow down AS progression [10].
Jonas Brinck, Karin Littmann and Magnus Bäck: Conceptualization; visualization; investigation; writing; editing and reviewing. Jonas Brinck and Magnus Bäck: Project administration and funding acquisition. Linnea Widman: Methodology/Statistics; reviewing. Daniel Eriksson Hogling, Kenneth Caidahl, Maria Eriksson and Karolina Szummer: Reviewing; editing. All authors approve the final version for publication and agree to be accountable for all aspects of the work.
JB reports institutional grants from Amgen, Novartis and Ionis outside the submitted work, and honoraria from Amgen, Novartis, Sanofi and Ultragenyx. DEH has received institutional honoraria from Amgen. KL reports research grant funding from Amgen and Stockholm Innovation Fund outside the submitted work and honoraria from Amgen and Sanofi. MBs’ institution has received speaker and consultant fees from Amarin, Amgen, Heel, Novartis and Fresenius Kabi. The remaining authors have nothing to disclose in relation to this work.
MB is supported by the Swedish Research Council, Grant Number: 2023-02652; Heart-Lung Foundation, Grant Number: 20240697.
The study was approved by the Ethical Review Authority.
期刊介绍:
JIM – The Journal of Internal Medicine, in continuous publication since 1863, is an international, peer-reviewed scientific journal. It publishes original work in clinical science, spanning from bench to bedside, encompassing a wide range of internal medicine and its subspecialties. JIM showcases original articles, reviews, brief reports, and research letters in the field of internal medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


