{"title":"二尖瓣反流的机制和病理生理:述评。","authors":"Praveen Kumar Neema, Nagarjuna Panidapu","doi":"10.4103/aca.aca_221_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>Mitral valve closure is a complex process and requires coordinated actions of all its interrelated anatomical components: the left atrium, the mitral annulus, the valve leaflets, the tendinous chordae, and the papillary muscles with its surrounding left ventricular wall for an effective mitral valve closure. Research of last three-decades has shown that the mitral annulus starts contracting during atrial systole which significantly prevent early mitral regurgitation (MR). MR can be acute or chronic, and primary, or secondary or mixed; their etiologies, mechanisms and natural progression are very different and have clinical implications. A leaflet perforation, a rupture of chorda tendinea or papillary muscle and a torn leaflet after balloon mitral valvotomy can result in acute severe MR. The patients of acute severe MR present in pulmonary edema and cardiogenic shock and often need urgent surgical intervention. Primary MR is a disease of the mitral valve apparatus and secondary to valve degeneration, whereas secondary MR is a disease of the left ventricle secondary to coronary artery disease and dilated cardiomyopathy. The other causes of secondary MR include mitral annular dilation secondary to atrial fibrillation and restrictive cardiomyopathy, dys-synchrony due to bundle branch block, right ventricular pacing and hypertrophic cardiomyopathy. The treatment strategy differs for primary and various subsets of secondary MR; hence, a thorough knowledge of the etiology, mechanisms and pathogenesis of MR is necessary to select appropriate management strategy and to decide when to intervene. The review discusses the mechanisms, and pathophysiology in acute, chronic, primary and secondary MR.</p>","PeriodicalId":7997,"journal":{"name":"Annals of Cardiac Anaesthesia","volume":"28 2","pages":"109-118"},"PeriodicalIF":1.3000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058057/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Mechanisms and Pathophysiology of Mitral Regurgitation: A Narrative Review.\",\"authors\":\"Praveen Kumar Neema, Nagarjuna Panidapu\",\"doi\":\"10.4103/aca.aca_221_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Abstract: </strong>Mitral valve closure is a complex process and requires coordinated actions of all its interrelated anatomical components: the left atrium, the mitral annulus, the valve leaflets, the tendinous chordae, and the papillary muscles with its surrounding left ventricular wall for an effective mitral valve closure. Research of last three-decades has shown that the mitral annulus starts contracting during atrial systole which significantly prevent early mitral regurgitation (MR). MR can be acute or chronic, and primary, or secondary or mixed; their etiologies, mechanisms and natural progression are very different and have clinical implications. A leaflet perforation, a rupture of chorda tendinea or papillary muscle and a torn leaflet after balloon mitral valvotomy can result in acute severe MR. The patients of acute severe MR present in pulmonary edema and cardiogenic shock and often need urgent surgical intervention. Primary MR is a disease of the mitral valve apparatus and secondary to valve degeneration, whereas secondary MR is a disease of the left ventricle secondary to coronary artery disease and dilated cardiomyopathy. The other causes of secondary MR include mitral annular dilation secondary to atrial fibrillation and restrictive cardiomyopathy, dys-synchrony due to bundle branch block, right ventricular pacing and hypertrophic cardiomyopathy. The treatment strategy differs for primary and various subsets of secondary MR; hence, a thorough knowledge of the etiology, mechanisms and pathogenesis of MR is necessary to select appropriate management strategy and to decide when to intervene. The review discusses the mechanisms, and pathophysiology in acute, chronic, primary and secondary MR.</p>\",\"PeriodicalId\":7997,\"journal\":{\"name\":\"Annals of Cardiac Anaesthesia\",\"volume\":\"28 2\",\"pages\":\"109-118\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058057/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Cardiac Anaesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/aca.aca_221_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Cardiac Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aca.aca_221_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
The Mechanisms and Pathophysiology of Mitral Regurgitation: A Narrative Review.
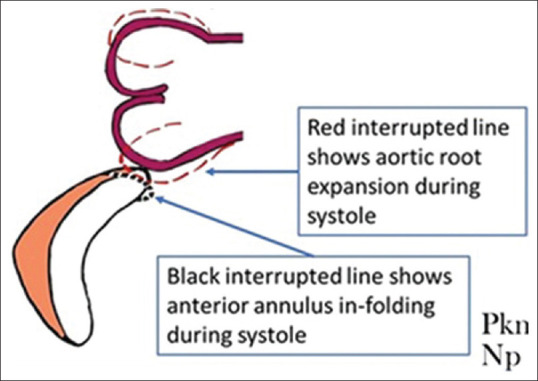
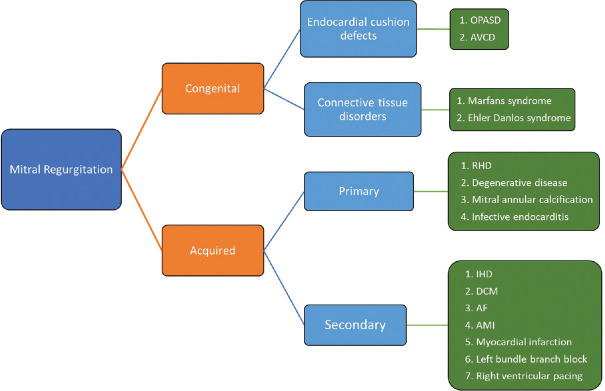
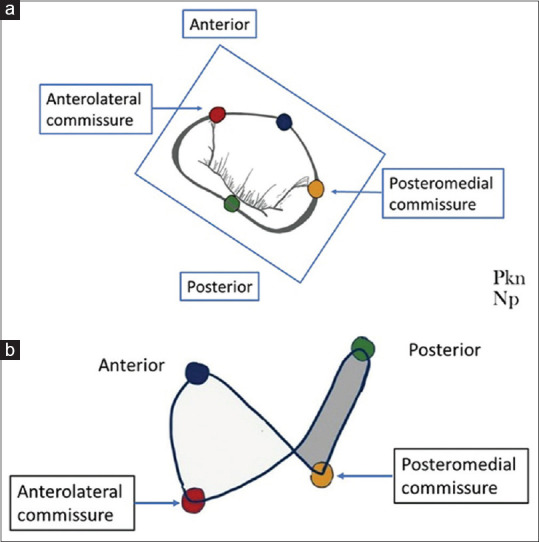
Abstract: Mitral valve closure is a complex process and requires coordinated actions of all its interrelated anatomical components: the left atrium, the mitral annulus, the valve leaflets, the tendinous chordae, and the papillary muscles with its surrounding left ventricular wall for an effective mitral valve closure. Research of last three-decades has shown that the mitral annulus starts contracting during atrial systole which significantly prevent early mitral regurgitation (MR). MR can be acute or chronic, and primary, or secondary or mixed; their etiologies, mechanisms and natural progression are very different and have clinical implications. A leaflet perforation, a rupture of chorda tendinea or papillary muscle and a torn leaflet after balloon mitral valvotomy can result in acute severe MR. The patients of acute severe MR present in pulmonary edema and cardiogenic shock and often need urgent surgical intervention. Primary MR is a disease of the mitral valve apparatus and secondary to valve degeneration, whereas secondary MR is a disease of the left ventricle secondary to coronary artery disease and dilated cardiomyopathy. The other causes of secondary MR include mitral annular dilation secondary to atrial fibrillation and restrictive cardiomyopathy, dys-synchrony due to bundle branch block, right ventricular pacing and hypertrophic cardiomyopathy. The treatment strategy differs for primary and various subsets of secondary MR; hence, a thorough knowledge of the etiology, mechanisms and pathogenesis of MR is necessary to select appropriate management strategy and to decide when to intervene. The review discusses the mechanisms, and pathophysiology in acute, chronic, primary and secondary MR.
期刊介绍:
Annals of Cardiac Anaesthesia (ACA) is the official journal of the Indian Association of Cardiovascular Thoracic Anaesthesiologists. The journal is indexed with PubMed/MEDLINE, Excerpta Medica/EMBASE, IndMed and MedInd. The journal’s full text is online at www.annals.in. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in ACA. Authors do not have to pay for submission, processing or publication of articles in ACA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


