Simon Schneekloth, Rasmus Paulin Beske, Johannes Grand, Jesper Kjaergaard, Jacob Eifer Møller, Henrik Schmidt, Anders Aneman, Christian Hassager
{"title":"心脏骤停后护理期间血压指标对静脉回流生理的影响。","authors":"Simon Schneekloth, Rasmus Paulin Beske, Johannes Grand, Jesper Kjaergaard, Jacob Eifer Møller, Henrik Schmidt, Anders Aneman, Christian Hassager","doi":"10.1111/aas.70038","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Venous return (VR) physiology may be elucidated using a calculated mean systemic filling pressure analogue (P<sub>msa</sub>) that reflects the stressed intravascular volume. The aim of this study was to explore differences in VR physiological variables with the hypothesis that vasopressor therapy targeting a higher mean arterial pressure (MAP) would associate with an increased volume state. This would be important to appreciate the intravascular volume effect of an intervention that traditionally is judged by the pressure response alone.</p><p><strong>Methods: </strong>This exploratory study used data from the BOX trial that investigated a higher (MAP of 77 mmHg, MAP77) versus a lower (63 mmHg, MAP63) blood pressure target during intensive care of survivors from out-of-hospital cardiac arrest. Data from 730 patients (MAP63, n = 362 and MAP77, n = 368) were used to calculate P<sub>msa</sub>, the driving pressure for VR (VRdP, the difference between P<sub>msa</sub> and central venous pressure [CVP]), the resistance to venous return (RVR, the VRdP divided by the cardiac output [CO]) and heart efficiency (E<sub>h</sub>, the VRdP divided by P<sub>msa</sub>). Linear mixed models were used to evaluate longitudinal haemodynamic data captured from admission to the intensive care unit and over 36 h.</p><p><strong>Results: </strong>The P<sub>msa</sub> was consistently higher in the MAP77 group (p < .03) while the CVP was not statistically different. The greater P<sub>msa</sub> translated into a progressively increasing VRdP (p < .0001) and thus an increased CO (p < .001). Similar stroke volumes in both groups meant that CO was maintained by an increased heart rate in MAP77 (p < .001). The RVR was higher in MAP77 (p < .04) but gradually decreased in both groups, while the E<sub>h</sub> was similar overall.</p><p><strong>Conclusion: </strong>In conclusion, a higher MAP target effectively increased the stressed intravascular volume to sustain a higher CO.</p><p><strong>Editorial comment: </strong>This post-hoc analysis of the BOX trial explores VR physiology and how it is influenced by the use of various doses of noradrenaline and dopamine. A higher blood pressure target appears to increase VR by increasing the stressed intravascular volume. This results in an increase in the CO. These findings are important given the worry about the effect of a higher afterload on cardiac function.</p>","PeriodicalId":6909,"journal":{"name":"Acta Anaesthesiologica Scandinavica","volume":"69 5","pages":"e70038"},"PeriodicalIF":2.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12004033/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact of blood pressure targets on venous return physiology during post cardiac arrest care.\",\"authors\":\"Simon Schneekloth, Rasmus Paulin Beske, Johannes Grand, Jesper Kjaergaard, Jacob Eifer Møller, Henrik Schmidt, Anders Aneman, Christian Hassager\",\"doi\":\"10.1111/aas.70038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Venous return (VR) physiology may be elucidated using a calculated mean systemic filling pressure analogue (P<sub>msa</sub>) that reflects the stressed intravascular volume. The aim of this study was to explore differences in VR physiological variables with the hypothesis that vasopressor therapy targeting a higher mean arterial pressure (MAP) would associate with an increased volume state. This would be important to appreciate the intravascular volume effect of an intervention that traditionally is judged by the pressure response alone.</p><p><strong>Methods: </strong>This exploratory study used data from the BOX trial that investigated a higher (MAP of 77 mmHg, MAP77) versus a lower (63 mmHg, MAP63) blood pressure target during intensive care of survivors from out-of-hospital cardiac arrest. Data from 730 patients (MAP63, n = 362 and MAP77, n = 368) were used to calculate P<sub>msa</sub>, the driving pressure for VR (VRdP, the difference between P<sub>msa</sub> and central venous pressure [CVP]), the resistance to venous return (RVR, the VRdP divided by the cardiac output [CO]) and heart efficiency (E<sub>h</sub>, the VRdP divided by P<sub>msa</sub>). Linear mixed models were used to evaluate longitudinal haemodynamic data captured from admission to the intensive care unit and over 36 h.</p><p><strong>Results: </strong>The P<sub>msa</sub> was consistently higher in the MAP77 group (p < .03) while the CVP was not statistically different. The greater P<sub>msa</sub> translated into a progressively increasing VRdP (p < .0001) and thus an increased CO (p < .001). Similar stroke volumes in both groups meant that CO was maintained by an increased heart rate in MAP77 (p < .001). The RVR was higher in MAP77 (p < .04) but gradually decreased in both groups, while the E<sub>h</sub> was similar overall.</p><p><strong>Conclusion: </strong>In conclusion, a higher MAP target effectively increased the stressed intravascular volume to sustain a higher CO.</p><p><strong>Editorial comment: </strong>This post-hoc analysis of the BOX trial explores VR physiology and how it is influenced by the use of various doses of noradrenaline and dopamine. A higher blood pressure target appears to increase VR by increasing the stressed intravascular volume. This results in an increase in the CO. These findings are important given the worry about the effect of a higher afterload on cardiac function.</p>\",\"PeriodicalId\":6909,\"journal\":{\"name\":\"Acta Anaesthesiologica Scandinavica\",\"volume\":\"69 5\",\"pages\":\"e70038\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12004033/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Anaesthesiologica Scandinavica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/aas.70038\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Anaesthesiologica Scandinavica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/aas.70038","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:静脉回流(VR)生理学可以通过计算的平均全身充盈压力模拟物(Pmsa)来阐明,该模拟物反映了受压的血管内容积。本研究的目的是探索VR生理变量的差异,并假设以更高的平均动脉压(MAP)为目标的血管加压治疗与容积状态的增加有关。传统上仅通过压力反应来判断干预措施的血管内容积效应,这将是很重要的。方法:本探索性研究使用BOX试验的数据,该试验调查了院外心脏骤停幸存者重症监护期间较高(MAP为77 mmHg, MAP77)与较低(63 mmHg, MAP63)的血压目标。730例患者(MAP63, n = 362, MAP77, n = 368)的数据用于计算Pmsa、VR驱动压(VRdP, Pmsa与中心静脉压之差[CVP])、静脉回流阻力(RVR, VRdP除以心输出量[CO])和心脏效率(Eh, VRdP除以Pmsa)。使用线性混合模型来评估从入院到重症监护病房36小时内捕获的纵向血流动力学数据。结果:MAP77组Pmsa持续升高(p msa转化为逐渐增加的VRdP) (p h总体相似。结论:总的来说,较高的MAP目标有效地增加了受压血管内容积,以维持较高的co .。编辑评论:BOX试验的事后分析探讨了VR生理学,以及使用不同剂量的去甲肾上腺素和多巴胺如何影响VR生理学。较高的血压目标似乎通过增加受压血管内容积来增加VR。这导致了CO的增加。考虑到高后负荷对心功能的影响,这些发现很重要。
The impact of blood pressure targets on venous return physiology during post cardiac arrest care.
Background: Venous return (VR) physiology may be elucidated using a calculated mean systemic filling pressure analogue (Pmsa) that reflects the stressed intravascular volume. The aim of this study was to explore differences in VR physiological variables with the hypothesis that vasopressor therapy targeting a higher mean arterial pressure (MAP) would associate with an increased volume state. This would be important to appreciate the intravascular volume effect of an intervention that traditionally is judged by the pressure response alone.
Methods: This exploratory study used data from the BOX trial that investigated a higher (MAP of 77 mmHg, MAP77) versus a lower (63 mmHg, MAP63) blood pressure target during intensive care of survivors from out-of-hospital cardiac arrest. Data from 730 patients (MAP63, n = 362 and MAP77, n = 368) were used to calculate Pmsa, the driving pressure for VR (VRdP, the difference between Pmsa and central venous pressure [CVP]), the resistance to venous return (RVR, the VRdP divided by the cardiac output [CO]) and heart efficiency (Eh, the VRdP divided by Pmsa). Linear mixed models were used to evaluate longitudinal haemodynamic data captured from admission to the intensive care unit and over 36 h.
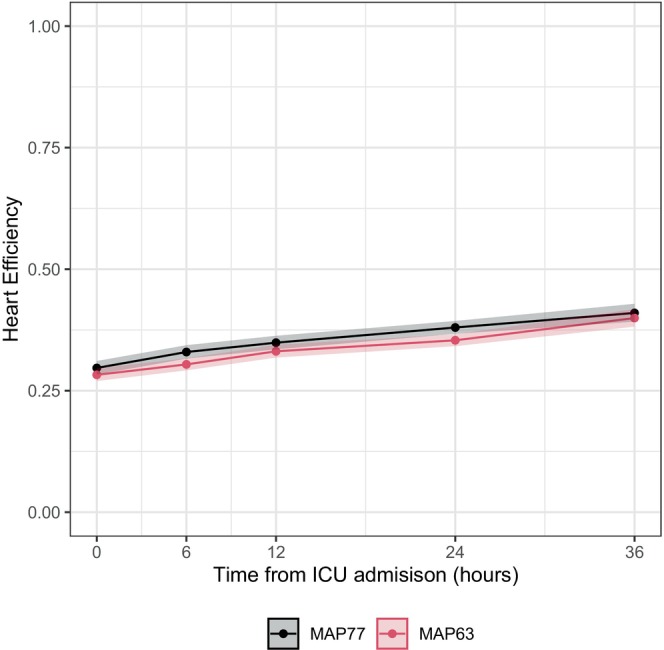
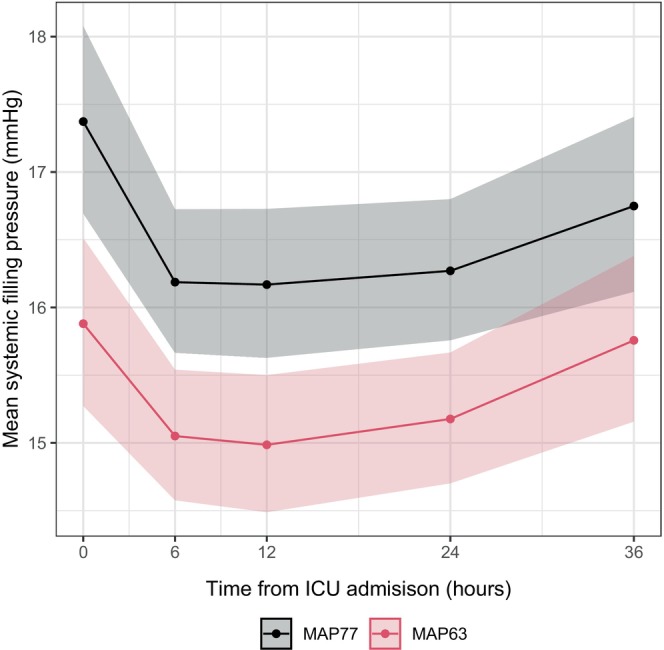
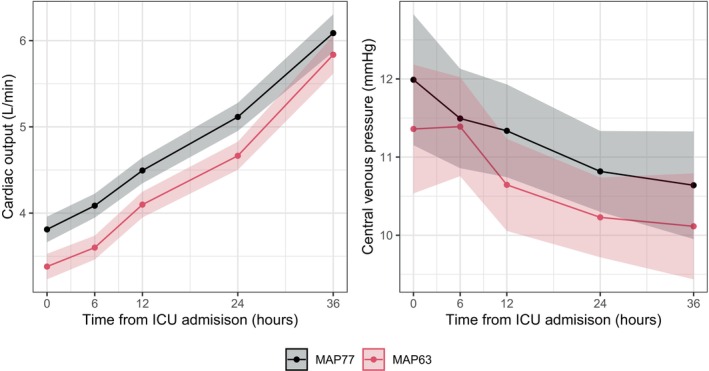
Results: The Pmsa was consistently higher in the MAP77 group (p < .03) while the CVP was not statistically different. The greater Pmsa translated into a progressively increasing VRdP (p < .0001) and thus an increased CO (p < .001). Similar stroke volumes in both groups meant that CO was maintained by an increased heart rate in MAP77 (p < .001). The RVR was higher in MAP77 (p < .04) but gradually decreased in both groups, while the Eh was similar overall.
Conclusion: In conclusion, a higher MAP target effectively increased the stressed intravascular volume to sustain a higher CO.
Editorial comment: This post-hoc analysis of the BOX trial explores VR physiology and how it is influenced by the use of various doses of noradrenaline and dopamine. A higher blood pressure target appears to increase VR by increasing the stressed intravascular volume. This results in an increase in the CO. These findings are important given the worry about the effect of a higher afterload on cardiac function.
期刊介绍:
Acta Anaesthesiologica Scandinavica publishes papers on original work in the fields of anaesthesiology, intensive care, pain, emergency medicine, and subjects related to their basic sciences, on condition that they are contributed exclusively to this Journal. Case reports and short communications may be considered for publication if of particular interest; also letters to the Editor, especially if related to already published material. The editorial board is free to discuss the publication of reviews on current topics, the choice of which, however, is the prerogative of the board. Every effort will be made by the Editors and selected experts to expedite a critical review of manuscripts in order to ensure rapid publication of papers of a high scientific standard.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


