Luxsena Sukumaran, Alan Winston, Jane Anderson, Marta Boffito, Frank A Post, Memory Sachikonye, Patrick W G Mallon, Laura Waters, Jaime Vera, Fiona Burns, Caroline A Sabin
{"title":"多发病框架影响模式的构成及其与艾滋病毒感染者患者报告结果的关联。","authors":"Luxsena Sukumaran, Alan Winston, Jane Anderson, Marta Boffito, Frank A Post, Memory Sachikonye, Patrick W G Mallon, Laura Waters, Jaime Vera, Fiona Burns, Caroline A Sabin","doi":"10.1177/26335565251331732","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives:</b> There is no consensus definition for multimorbidity. We explored how different frameworks affect multimorbidity patterns and their associations with patient-reported outcomes using the prospective, observational Pharmacokinetic and clinical Observations in PeoPle over fiftY (POPPY) Study. <b>Methods:</b> Sixty-four conditions were classified into three frameworks: Framework-D (diseases), Framework-DCI (diseases and clinical indicators) and Framework-DCIS (diseases, clinical indicators and symptoms). Principal component analysis (PCA) identified five comparable patterns: <i>Cardiovascular disease (CVD)</i>, <i>Sexually transmitted diseases</i>, <i>Metabolic/AIDS-related</i>, <i>Mental health/Other</i>, and <i>Cancer</i>. A sixth pattern was identified using Framework-D (<i>Infections/Skin)</i> and Framework-DCI/DCIS (<i>Cardiometabolic)</i>. Using PCA loadings, burden z-scores were calculated for each individual/pattern, and their associations with functional impairment (Lawton Instrumental Activities of Daily Living <8), hospitalisation and SF-36 physical and mental health scores were assessed using logistic or linear regression. <b>Results:</b> The analyses included 1073 people with HIV (median [interquartile range; IQR] age 52 [47 - 59] years; 85% male; 97% on ART). Clinical indicators and symptoms were correlated with the <i>CVD</i>, <i>Cardiometabolic</i> and <i>Mental health/Other</i> patterns. While differences were marginal, Framework-DCI showed slightly stronger relationships between <i>CVD</i> and functional impairment, hospitalisation and physical health compared to Framework-D. Similarly, Framework-DCIS demonstrated somewhat stronger associations between <i>Metabolic/AIDS-related</i> and <i>Mental health/Other</i> patterns with certain outcomes. <b>Conclusions:</b> The inclusion of clinical indicators and symptoms were associated with some changes in the strength of associations between certain multimorbidity patterns and outcomes. Our findings suggest that their inclusion in multimorbidity frameworks should be guided by the specific research context and question, rather than solely by effect size on patient-important outcomes.</p>","PeriodicalId":73843,"journal":{"name":"Journal of multimorbidity and comorbidity","volume":"15 ","pages":"26335565251331732"},"PeriodicalIF":3.0000,"publicationDate":"2025-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11970071/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multimorbidity frameworks impact the composition of patterns and their associations with patient-reported outcomes among people with HIV.\",\"authors\":\"Luxsena Sukumaran, Alan Winston, Jane Anderson, Marta Boffito, Frank A Post, Memory Sachikonye, Patrick W G Mallon, Laura Waters, Jaime Vera, Fiona Burns, Caroline A Sabin\",\"doi\":\"10.1177/26335565251331732\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Objectives:</b> There is no consensus definition for multimorbidity. We explored how different frameworks affect multimorbidity patterns and their associations with patient-reported outcomes using the prospective, observational Pharmacokinetic and clinical Observations in PeoPle over fiftY (POPPY) Study. <b>Methods:</b> Sixty-four conditions were classified into three frameworks: Framework-D (diseases), Framework-DCI (diseases and clinical indicators) and Framework-DCIS (diseases, clinical indicators and symptoms). Principal component analysis (PCA) identified five comparable patterns: <i>Cardiovascular disease (CVD)</i>, <i>Sexually transmitted diseases</i>, <i>Metabolic/AIDS-related</i>, <i>Mental health/Other</i>, and <i>Cancer</i>. A sixth pattern was identified using Framework-D (<i>Infections/Skin)</i> and Framework-DCI/DCIS (<i>Cardiometabolic)</i>. Using PCA loadings, burden z-scores were calculated for each individual/pattern, and their associations with functional impairment (Lawton Instrumental Activities of Daily Living <8), hospitalisation and SF-36 physical and mental health scores were assessed using logistic or linear regression. <b>Results:</b> The analyses included 1073 people with HIV (median [interquartile range; IQR] age 52 [47 - 59] years; 85% male; 97% on ART). Clinical indicators and symptoms were correlated with the <i>CVD</i>, <i>Cardiometabolic</i> and <i>Mental health/Other</i> patterns. While differences were marginal, Framework-DCI showed slightly stronger relationships between <i>CVD</i> and functional impairment, hospitalisation and physical health compared to Framework-D. Similarly, Framework-DCIS demonstrated somewhat stronger associations between <i>Metabolic/AIDS-related</i> and <i>Mental health/Other</i> patterns with certain outcomes. <b>Conclusions:</b> The inclusion of clinical indicators and symptoms were associated with some changes in the strength of associations between certain multimorbidity patterns and outcomes. Our findings suggest that their inclusion in multimorbidity frameworks should be guided by the specific research context and question, rather than solely by effect size on patient-important outcomes.</p>\",\"PeriodicalId\":73843,\"journal\":{\"name\":\"Journal of multimorbidity and comorbidity\",\"volume\":\"15 \",\"pages\":\"26335565251331732\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-04-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11970071/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of multimorbidity and comorbidity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26335565251331732\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of multimorbidity and comorbidity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26335565251331732","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Multimorbidity frameworks impact the composition of patterns and their associations with patient-reported outcomes among people with HIV.
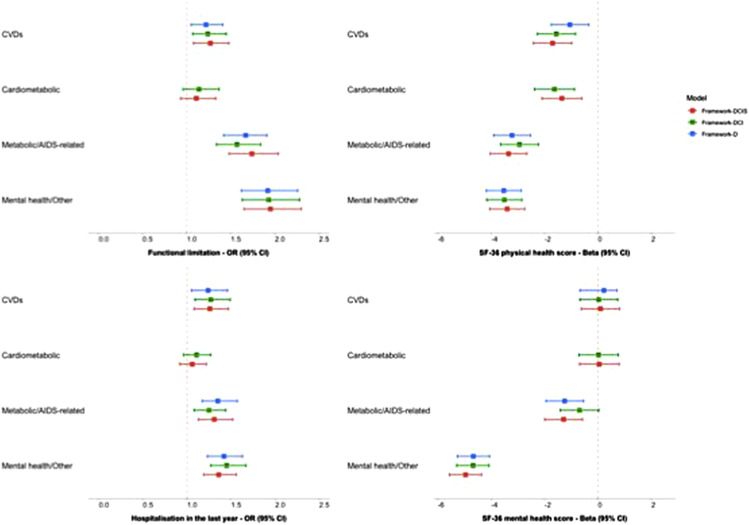
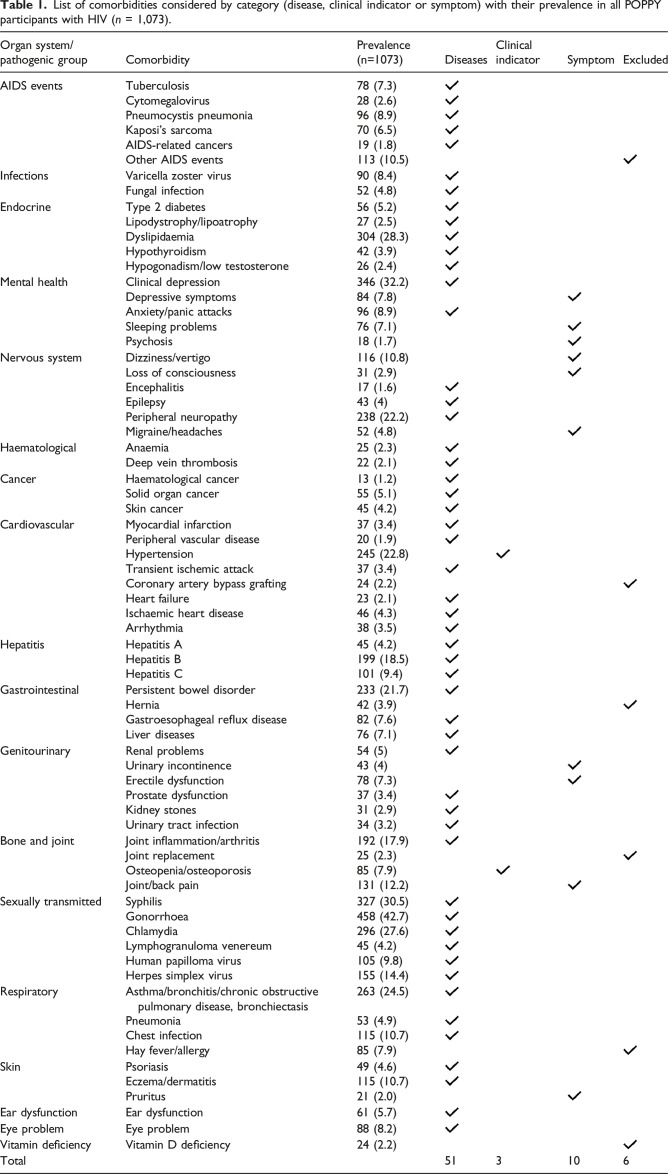
Objectives: There is no consensus definition for multimorbidity. We explored how different frameworks affect multimorbidity patterns and their associations with patient-reported outcomes using the prospective, observational Pharmacokinetic and clinical Observations in PeoPle over fiftY (POPPY) Study. Methods: Sixty-four conditions were classified into three frameworks: Framework-D (diseases), Framework-DCI (diseases and clinical indicators) and Framework-DCIS (diseases, clinical indicators and symptoms). Principal component analysis (PCA) identified five comparable patterns: Cardiovascular disease (CVD), Sexually transmitted diseases, Metabolic/AIDS-related, Mental health/Other, and Cancer. A sixth pattern was identified using Framework-D (Infections/Skin) and Framework-DCI/DCIS (Cardiometabolic). Using PCA loadings, burden z-scores were calculated for each individual/pattern, and their associations with functional impairment (Lawton Instrumental Activities of Daily Living <8), hospitalisation and SF-36 physical and mental health scores were assessed using logistic or linear regression. Results: The analyses included 1073 people with HIV (median [interquartile range; IQR] age 52 [47 - 59] years; 85% male; 97% on ART). Clinical indicators and symptoms were correlated with the CVD, Cardiometabolic and Mental health/Other patterns. While differences were marginal, Framework-DCI showed slightly stronger relationships between CVD and functional impairment, hospitalisation and physical health compared to Framework-D. Similarly, Framework-DCIS demonstrated somewhat stronger associations between Metabolic/AIDS-related and Mental health/Other patterns with certain outcomes. Conclusions: The inclusion of clinical indicators and symptoms were associated with some changes in the strength of associations between certain multimorbidity patterns and outcomes. Our findings suggest that their inclusion in multimorbidity frameworks should be guided by the specific research context and question, rather than solely by effect size on patient-important outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


