{"title":"早期胰岛素可避免慢发杜伐单抗诱导的检查点抑制剂相关自身免疫性糖尿病的高血糖危机","authors":"Takaaki Matsuda, Yoshinori Osaki, Motohiro Sekiya, Hitoshi Shimano","doi":"10.2185/jrm.2024-030","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Checkpoint inhibitor-associated autoimmune diabetes mellitus (CIADM), a variant of type 1 diabetes, is a rare immune-related adverse events (irAEs) caused by antibody-based immune checkpoint inhibitors. CIADM typically manifests as fulminant or acute-onset type 1 diabetes in the insulin-depleted state. However, we encountered a patient with slow-onset CIADM who initially presented with hyperglycemia without decreased insulin secretion after treatment with durvalumab (an anti-PD-L1 antibody).</p><p><strong>Patient: </strong>A 60-year-old man diagnosed with small-cell lung cancer on durvalumab combined with dexamethasone treatment experienced an increase in glycated hemoglobin (HbA1c) from 6.4% to 7.8% after three cycles.</p><p><strong>Results: </strong>Despite preserved endogenous insulin secretion (C-peptide, 2.47 ng/mL with a casual plasma glucose level of 287 mg/dL), basal insulin therapy was initiated considering CIADM. HbA1c levels remained stable (8.5-9.2%) for 3 months but increased to 13.4% at 18 weeks, indicative of CIADM. Declining endogenous insulin secretion resulted in ketosis; however, hyperglycemic crisis was prevented through basal insulin therapy.</p><p><strong>Conclusion: </strong>We emphasize that CIADM develops gradually and does not always occur in the course of fulminant or acute-onset type 1 diabetes; therefore, early initiation of insulin in the presence of hyperglycemia is crucial to prevent hyperglycemic crises.</p>","PeriodicalId":73939,"journal":{"name":"Journal of rural medicine : JRM","volume":"20 2","pages":"150-155"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11962188/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early insulin averts hyperglycemic crisis in slow-onset durvalumab-induced checkpoint inhibitor-associated autoimmune diabetes mellitus.\",\"authors\":\"Takaaki Matsuda, Yoshinori Osaki, Motohiro Sekiya, Hitoshi Shimano\",\"doi\":\"10.2185/jrm.2024-030\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Checkpoint inhibitor-associated autoimmune diabetes mellitus (CIADM), a variant of type 1 diabetes, is a rare immune-related adverse events (irAEs) caused by antibody-based immune checkpoint inhibitors. CIADM typically manifests as fulminant or acute-onset type 1 diabetes in the insulin-depleted state. However, we encountered a patient with slow-onset CIADM who initially presented with hyperglycemia without decreased insulin secretion after treatment with durvalumab (an anti-PD-L1 antibody).</p><p><strong>Patient: </strong>A 60-year-old man diagnosed with small-cell lung cancer on durvalumab combined with dexamethasone treatment experienced an increase in glycated hemoglobin (HbA1c) from 6.4% to 7.8% after three cycles.</p><p><strong>Results: </strong>Despite preserved endogenous insulin secretion (C-peptide, 2.47 ng/mL with a casual plasma glucose level of 287 mg/dL), basal insulin therapy was initiated considering CIADM. HbA1c levels remained stable (8.5-9.2%) for 3 months but increased to 13.4% at 18 weeks, indicative of CIADM. Declining endogenous insulin secretion resulted in ketosis; however, hyperglycemic crisis was prevented through basal insulin therapy.</p><p><strong>Conclusion: </strong>We emphasize that CIADM develops gradually and does not always occur in the course of fulminant or acute-onset type 1 diabetes; therefore, early initiation of insulin in the presence of hyperglycemia is crucial to prevent hyperglycemic crises.</p>\",\"PeriodicalId\":73939,\"journal\":{\"name\":\"Journal of rural medicine : JRM\",\"volume\":\"20 2\",\"pages\":\"150-155\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11962188/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of rural medicine : JRM\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2185/jrm.2024-030\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of rural medicine : JRM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2185/jrm.2024-030","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Early insulin averts hyperglycemic crisis in slow-onset durvalumab-induced checkpoint inhibitor-associated autoimmune diabetes mellitus.
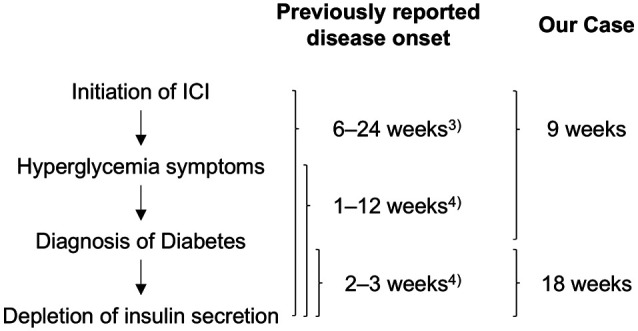
Objective: Checkpoint inhibitor-associated autoimmune diabetes mellitus (CIADM), a variant of type 1 diabetes, is a rare immune-related adverse events (irAEs) caused by antibody-based immune checkpoint inhibitors. CIADM typically manifests as fulminant or acute-onset type 1 diabetes in the insulin-depleted state. However, we encountered a patient with slow-onset CIADM who initially presented with hyperglycemia without decreased insulin secretion after treatment with durvalumab (an anti-PD-L1 antibody).
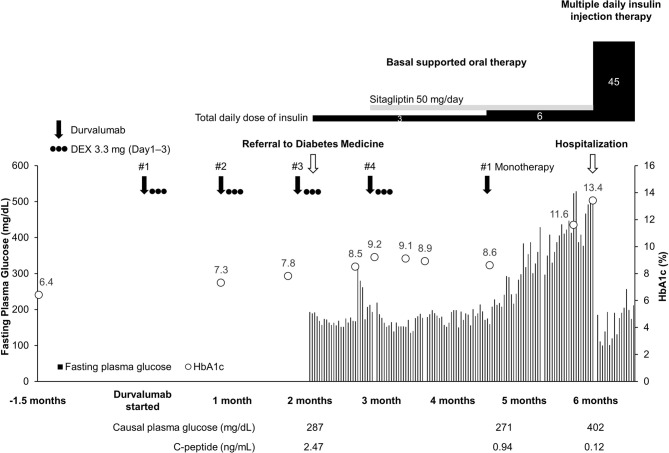
Patient: A 60-year-old man diagnosed with small-cell lung cancer on durvalumab combined with dexamethasone treatment experienced an increase in glycated hemoglobin (HbA1c) from 6.4% to 7.8% after three cycles.
Results: Despite preserved endogenous insulin secretion (C-peptide, 2.47 ng/mL with a casual plasma glucose level of 287 mg/dL), basal insulin therapy was initiated considering CIADM. HbA1c levels remained stable (8.5-9.2%) for 3 months but increased to 13.4% at 18 weeks, indicative of CIADM. Declining endogenous insulin secretion resulted in ketosis; however, hyperglycemic crisis was prevented through basal insulin therapy.
Conclusion: We emphasize that CIADM develops gradually and does not always occur in the course of fulminant or acute-onset type 1 diabetes; therefore, early initiation of insulin in the presence of hyperglycemia is crucial to prevent hyperglycemic crises.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


