Khanyisile M Tshabalala, Inger Fabris-Rotelli, Debashis Basu, Magriet Myburgh, Fareed Abdullah
{"title":"2019冠状病毒病之前和期间南非一家医院的死亡率趋势和死亡原因","authors":"Khanyisile M Tshabalala, Inger Fabris-Rotelli, Debashis Basu, Magriet Myburgh, Fareed Abdullah","doi":"10.4102/sajid.v40i1.679","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Before coronavirus disease 2019 (COVID-19), global health was improving, with declining mortality trends. The pandemic disrupted this progress, increasing mortality in South Africa between April 2020 and March 2022. Pre-pandemic data establishes a baseline for assessing COVID-19's impact on all-cause mortality.</p><p><strong>Objectives: </strong>This study examines changes in hospital-based mortality trends in a Gauteng hospital complex from April 2018 to March 2022, addressing the scarcity of such studies during the COVID-19 era.</p><p><strong>Method: </strong>A retrospective review of 7815 deaths from April 2018 to March 2022 was conducted. Chi-squared tests were used to analyse deaths by age group and gender, with correlations reported.</p><p><strong>Results: </strong>Mortality rates rose from 3.2% in 2018-2019, peaked at 5.1% in 2020-2021, and declined to 4.2% in 2021-2022. Patients aged 15 years-64 years had the highest death rates, with an increase among those over 65. Male deaths exceeded female deaths, with the smallest difference observed in 2020-2021. Leading causes of death included diseases of the circulatory and respiratory systems, neoplasms, digestive system diseases, and infectious and parasitic diseases.</p><p><strong>Conclusion: </strong>The study highlights COVID-19's impact on mortality, showing variations by year, age, gender, and disease.</p><p><strong>Contribution: </strong>Excess non-COVID-19 deaths likely stemmed from disrupted healthcare services. These findings underscore the need for ongoing monitoring of hospital mortality to identify pandemic-related service disruptions and guide interventions to strengthen healthcare services, improve access to care, and enhance referral systems during unexpected disasters.</p>","PeriodicalId":44007,"journal":{"name":"Southern African Journal of Infectious Diseases","volume":"40 1","pages":"679"},"PeriodicalIF":1.3000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11966701/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mortality trends and causes of death in a South African hospital complex pre- and during COVID-19.\",\"authors\":\"Khanyisile M Tshabalala, Inger Fabris-Rotelli, Debashis Basu, Magriet Myburgh, Fareed Abdullah\",\"doi\":\"10.4102/sajid.v40i1.679\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Before coronavirus disease 2019 (COVID-19), global health was improving, with declining mortality trends. The pandemic disrupted this progress, increasing mortality in South Africa between April 2020 and March 2022. Pre-pandemic data establishes a baseline for assessing COVID-19's impact on all-cause mortality.</p><p><strong>Objectives: </strong>This study examines changes in hospital-based mortality trends in a Gauteng hospital complex from April 2018 to March 2022, addressing the scarcity of such studies during the COVID-19 era.</p><p><strong>Method: </strong>A retrospective review of 7815 deaths from April 2018 to March 2022 was conducted. Chi-squared tests were used to analyse deaths by age group and gender, with correlations reported.</p><p><strong>Results: </strong>Mortality rates rose from 3.2% in 2018-2019, peaked at 5.1% in 2020-2021, and declined to 4.2% in 2021-2022. Patients aged 15 years-64 years had the highest death rates, with an increase among those over 65. Male deaths exceeded female deaths, with the smallest difference observed in 2020-2021. Leading causes of death included diseases of the circulatory and respiratory systems, neoplasms, digestive system diseases, and infectious and parasitic diseases.</p><p><strong>Conclusion: </strong>The study highlights COVID-19's impact on mortality, showing variations by year, age, gender, and disease.</p><p><strong>Contribution: </strong>Excess non-COVID-19 deaths likely stemmed from disrupted healthcare services. These findings underscore the need for ongoing monitoring of hospital mortality to identify pandemic-related service disruptions and guide interventions to strengthen healthcare services, improve access to care, and enhance referral systems during unexpected disasters.</p>\",\"PeriodicalId\":44007,\"journal\":{\"name\":\"Southern African Journal of Infectious Diseases\",\"volume\":\"40 1\",\"pages\":\"679\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-03-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11966701/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Southern African Journal of Infectious Diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4102/sajid.v40i1.679\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Southern African Journal of Infectious Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/sajid.v40i1.679","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Mortality trends and causes of death in a South African hospital complex pre- and during COVID-19.
Background: Before coronavirus disease 2019 (COVID-19), global health was improving, with declining mortality trends. The pandemic disrupted this progress, increasing mortality in South Africa between April 2020 and March 2022. Pre-pandemic data establishes a baseline for assessing COVID-19's impact on all-cause mortality.
Objectives: This study examines changes in hospital-based mortality trends in a Gauteng hospital complex from April 2018 to March 2022, addressing the scarcity of such studies during the COVID-19 era.
Method: A retrospective review of 7815 deaths from April 2018 to March 2022 was conducted. Chi-squared tests were used to analyse deaths by age group and gender, with correlations reported.
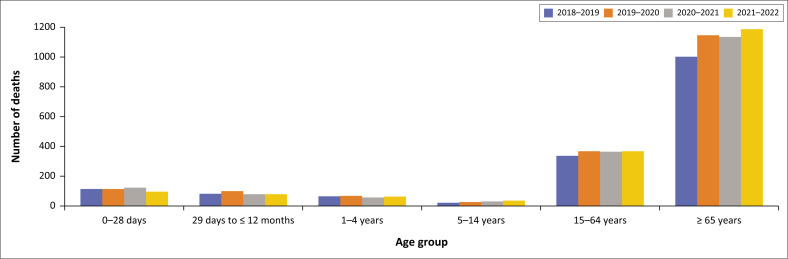
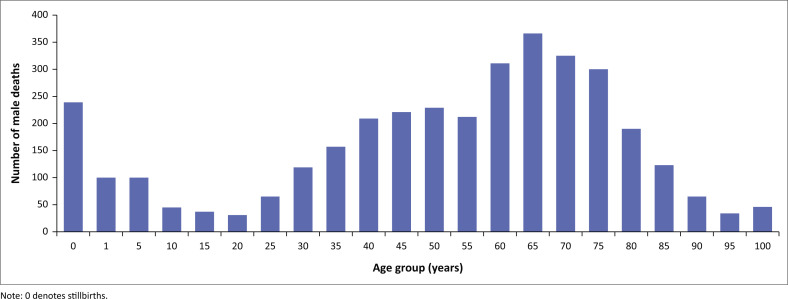
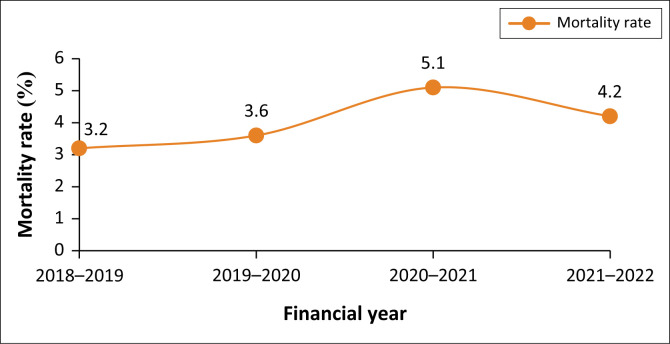
Results: Mortality rates rose from 3.2% in 2018-2019, peaked at 5.1% in 2020-2021, and declined to 4.2% in 2021-2022. Patients aged 15 years-64 years had the highest death rates, with an increase among those over 65. Male deaths exceeded female deaths, with the smallest difference observed in 2020-2021. Leading causes of death included diseases of the circulatory and respiratory systems, neoplasms, digestive system diseases, and infectious and parasitic diseases.
Conclusion: The study highlights COVID-19's impact on mortality, showing variations by year, age, gender, and disease.
Contribution: Excess non-COVID-19 deaths likely stemmed from disrupted healthcare services. These findings underscore the need for ongoing monitoring of hospital mortality to identify pandemic-related service disruptions and guide interventions to strengthen healthcare services, improve access to care, and enhance referral systems during unexpected disasters.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


