Joanie Martineau, Francis Bernard, Alexandrine Gagnon, Virginie Williams, Sabrina Araujo de Franca, David Williamson, Yiorgos Alexandros Cavayas
{"title":"在急性脑损伤的重症患者中,动脉二氧化碳的变化比其同步值更能决定脑组织氧合。","authors":"Joanie Martineau, Francis Bernard, Alexandrine Gagnon, Virginie Williams, Sabrina Araujo de Franca, David Williamson, Yiorgos Alexandros Cavayas","doi":"10.1097/CCE.0000000000001241","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>In critically ill patients with acute brain injury (ABI), maintaining intracranial pressure (ICP) and brain tissue oxygenation (PbtO2) within targets could prevent secondary neurologic injury. Tight control of CO2 (Paco2), a potent regulator of cerebrovascular tone, is generally advocated, but its vasomotor effect may be short-lived. Our aim was to compare the effect of the synchronous Paco2 vs. its variation from a previous baseline on PbtO2 and ICP.</p><p><strong>Design: </strong>We performed a post hoc analysis of a prospective cohort study collecting arterial blood gas (ABG) values alongside synchronous neuromonitoring variables. Linear mixed-effects models were fitted to evaluate the association between Paco2 and/or Paco2 variation from its average of the last 8-24 hr vs. PbtO2 and ICP, while controlling for cerebral perfusion pressure and Pao2.</p><p><strong>Setting: </strong>Mixed medical-surgical ICU of Sacré-Coeur Hospital, an academic trauma center in Montreal, Canada.</p><p><strong>Patients: </strong>All consecutive adult patients admitted for ABI with ICP and PbtO2 monitoring between May 2017 and November 2021.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>We included 78 patients with 3047 ABG-neuromonitoring couplets. The model using the variation of Paco2 from its average of the last 24 hr displayed the best performance for the prediction of PbtO2 (coefficient 0.37; 95% CI 0.21-0.53). The strongest predictor of ICP was the variation of Paco2 from its average of the last 8 hr (coefficient 0.17; 95% CI 0.10-0.23).</p><p><strong>Conclusions: </strong>Variation in Paco2 from baseline is a more significant determinant of PbtO2 and ICP than the absolute Paco2 value at a given time. There may be a baseline vasomotor reset when patients are exposed to a given level of CO2 for 8 to 24 hr. Therefore, sustained intentional manipulation of Paco2 is unlikely to have lasting effects and slower correction rates of high or low Paco2 could help prevent brain tissue hypoxia or intracranial hypertension, respectively.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 4","pages":"e1241"},"PeriodicalIF":2.7000,"publicationDate":"2025-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968020/pdf/","citationCount":"0","resultStr":"{\"title\":\"Variation in Arterial CO2 is a Stronger Determinant of Brain Tissue Oxygenation Than its Synchronous Value in Critically Ill Patients With Acute Brain Injury.\",\"authors\":\"Joanie Martineau, Francis Bernard, Alexandrine Gagnon, Virginie Williams, Sabrina Araujo de Franca, David Williamson, Yiorgos Alexandros Cavayas\",\"doi\":\"10.1097/CCE.0000000000001241\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>In critically ill patients with acute brain injury (ABI), maintaining intracranial pressure (ICP) and brain tissue oxygenation (PbtO2) within targets could prevent secondary neurologic injury. Tight control of CO2 (Paco2), a potent regulator of cerebrovascular tone, is generally advocated, but its vasomotor effect may be short-lived. Our aim was to compare the effect of the synchronous Paco2 vs. its variation from a previous baseline on PbtO2 and ICP.</p><p><strong>Design: </strong>We performed a post hoc analysis of a prospective cohort study collecting arterial blood gas (ABG) values alongside synchronous neuromonitoring variables. Linear mixed-effects models were fitted to evaluate the association between Paco2 and/or Paco2 variation from its average of the last 8-24 hr vs. PbtO2 and ICP, while controlling for cerebral perfusion pressure and Pao2.</p><p><strong>Setting: </strong>Mixed medical-surgical ICU of Sacré-Coeur Hospital, an academic trauma center in Montreal, Canada.</p><p><strong>Patients: </strong>All consecutive adult patients admitted for ABI with ICP and PbtO2 monitoring between May 2017 and November 2021.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>We included 78 patients with 3047 ABG-neuromonitoring couplets. The model using the variation of Paco2 from its average of the last 24 hr displayed the best performance for the prediction of PbtO2 (coefficient 0.37; 95% CI 0.21-0.53). The strongest predictor of ICP was the variation of Paco2 from its average of the last 8 hr (coefficient 0.17; 95% CI 0.10-0.23).</p><p><strong>Conclusions: </strong>Variation in Paco2 from baseline is a more significant determinant of PbtO2 and ICP than the absolute Paco2 value at a given time. There may be a baseline vasomotor reset when patients are exposed to a given level of CO2 for 8 to 24 hr. Therefore, sustained intentional manipulation of Paco2 is unlikely to have lasting effects and slower correction rates of high or low Paco2 could help prevent brain tissue hypoxia or intracranial hypertension, respectively.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 4\",\"pages\":\"e1241\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968020/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001241\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001241","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
目的:在重症急性脑损伤(ABI)患者中,维持颅内压(ICP)和脑组织氧合(PbtO2)在目标范围内可预防继发性神经系统损伤。严格控制二氧化碳(Paco2)是脑血管张力的有效调节剂,通常被提倡,但其血管舒缩作用可能是短暂的。我们的目的是比较同步Paco2与之前基线的变化对PbtO2和ICP的影响。设计:我们对一项前瞻性队列研究进行了事后分析,该研究收集了动脉血气(ABG)值以及同步神经监测变量。在控制脑灌注压和Pao2的情况下,拟合线性混合效应模型来评估Paco2和/或Paco2在过去8-24小时的平均值变化与PbtO2和ICP之间的关系。地点:加拿大蒙特利尔的学术创伤中心sacr - coeur医院的综合内科-外科ICU。患者:2017年5月至2021年11月期间,所有连续因ABI入院并进行ICP和PbtO2监测的成年患者。干预措施:没有。测量和主要结果:我们纳入了78例3047例abg -神经监测联。利用Paco2过去24小时平均值变化的模型对PbtO2的预测效果最好(系数0.37;95% ci 0.21-0.53)。ICP的最强预测因子是Paco2相对于前8小时平均值的变化(系数0.17;95% ci 0.10-0.23)。结论:与基线相比,Paco2的变化是PbtO2和ICP的一个更重要的决定因素,而不是给定时间的绝对Paco2值。当患者暴露于给定水平的二氧化碳8至24小时时,可能会出现基线血管舒缩复位。因此,持续的故意操作Paco2不太可能产生持久的效果,较慢的高或低Paco2矫正率分别有助于预防脑组织缺氧或颅内高压。
Variation in Arterial CO2 is a Stronger Determinant of Brain Tissue Oxygenation Than its Synchronous Value in Critically Ill Patients With Acute Brain Injury.
Objectives: In critically ill patients with acute brain injury (ABI), maintaining intracranial pressure (ICP) and brain tissue oxygenation (PbtO2) within targets could prevent secondary neurologic injury. Tight control of CO2 (Paco2), a potent regulator of cerebrovascular tone, is generally advocated, but its vasomotor effect may be short-lived. Our aim was to compare the effect of the synchronous Paco2 vs. its variation from a previous baseline on PbtO2 and ICP.
Design: We performed a post hoc analysis of a prospective cohort study collecting arterial blood gas (ABG) values alongside synchronous neuromonitoring variables. Linear mixed-effects models were fitted to evaluate the association between Paco2 and/or Paco2 variation from its average of the last 8-24 hr vs. PbtO2 and ICP, while controlling for cerebral perfusion pressure and Pao2.
Setting: Mixed medical-surgical ICU of Sacré-Coeur Hospital, an academic trauma center in Montreal, Canada.
Patients: All consecutive adult patients admitted for ABI with ICP and PbtO2 monitoring between May 2017 and November 2021.
Interventions: None.
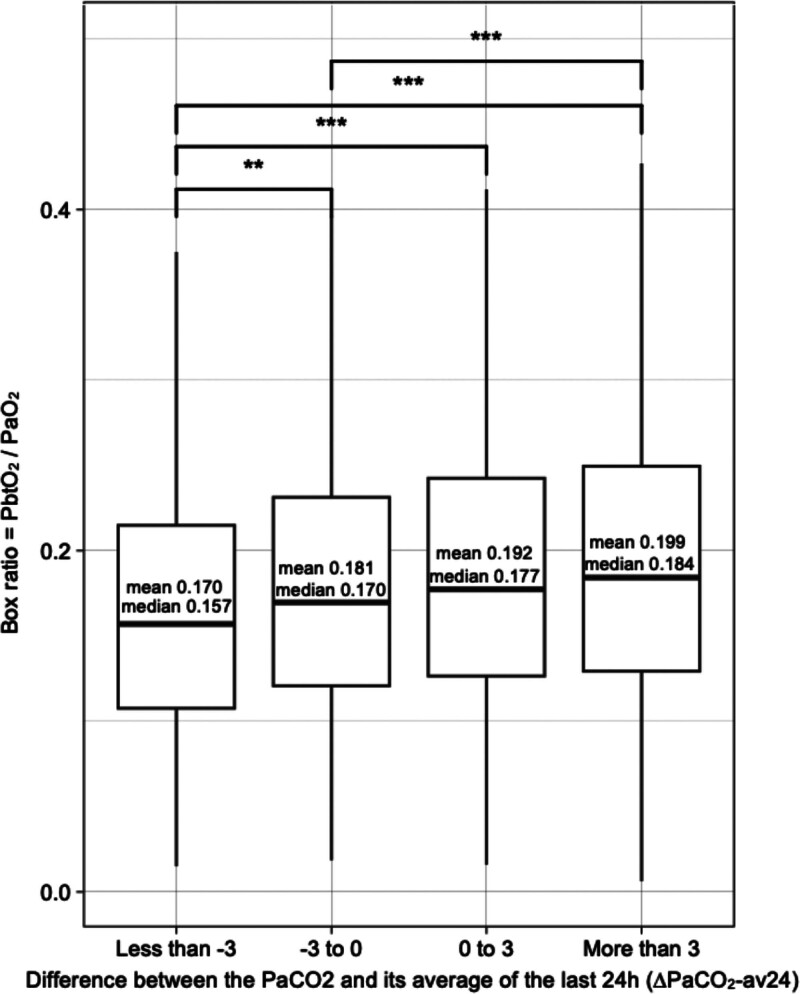
Measurements and main results: We included 78 patients with 3047 ABG-neuromonitoring couplets. The model using the variation of Paco2 from its average of the last 24 hr displayed the best performance for the prediction of PbtO2 (coefficient 0.37; 95% CI 0.21-0.53). The strongest predictor of ICP was the variation of Paco2 from its average of the last 8 hr (coefficient 0.17; 95% CI 0.10-0.23).
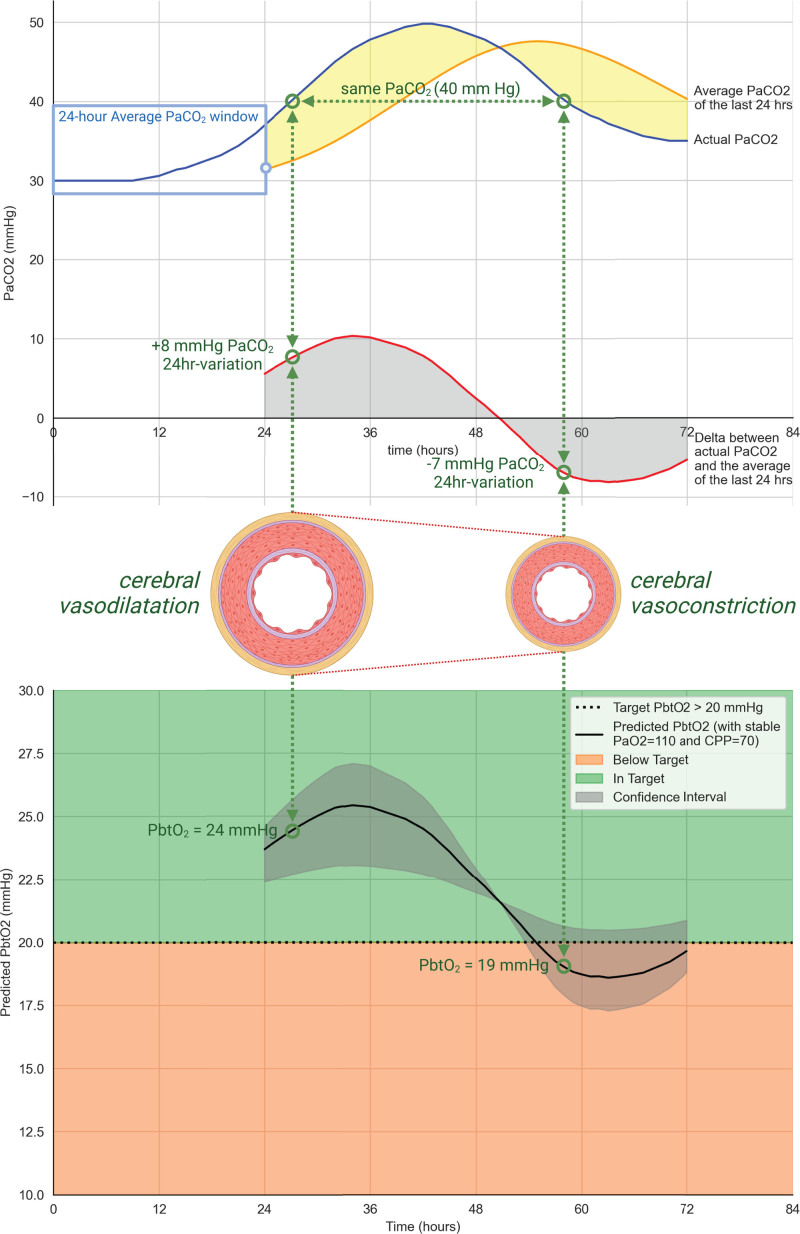
Conclusions: Variation in Paco2 from baseline is a more significant determinant of PbtO2 and ICP than the absolute Paco2 value at a given time. There may be a baseline vasomotor reset when patients are exposed to a given level of CO2 for 8 to 24 hr. Therefore, sustained intentional manipulation of Paco2 is unlikely to have lasting effects and slower correction rates of high or low Paco2 could help prevent brain tissue hypoxia or intracranial hypertension, respectively.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


