{"title":"心电测量治疗小儿感染性休克:一项随机对照试验。","authors":"Suman Sudha Moharana, Lalitha Av, Santu Ghosh","doi":"10.1097/CCE.0000000000001242","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the difference in the resuscitation fluid volume in the initial 6 hours in pediatric septic shock between those undergoing noninvasive continuous hemodynamic monitoring with electrocardiometry in addition to clinical monitoring vs. clinical monitoring alone.</p><p><strong>Design: </strong>Randomized control trial.</p><p><strong>Setting: </strong>PICU in a tertiary care hospital.</p><p><strong>Patients: </strong>Children from 2 months to 18 years with sepsis and unresolved shock after the initial fluid bolus (FB).</p><p><strong>Interventions: </strong>Children were randomized to one of the two groups, that is, electrocardiometry with clinical monitoring group (group B) and clinical monitoring alone group (group A). In group B, electrocardiometry variables (cardiac index and systemic vascular resistance index) along with clinical monitoring were used to guide FB, as well as selection and titration of vasoactive agents. Clinical parameters were used to initiate and titrate fluid resuscitation and vasoactive therapy in group A as per standard guidelines.</p><p><strong>Measurements and main results: </strong>One hundred nineteen children were enrolled in the study: 60 in group A and 59 in group B. There was a significantly higher requirement for resuscitation fluid volume (mean ± sd) within the initial 6 hours in the group A (30 ± 8.2 mL/kg) as compared with group B (22 ± 9.2 mL/kg). Similarly, maintenance along with resuscitation fluid volume (mean ± sd) administration (56 ±13 vs. 46 ±10.7, p < 0.001) was higher in group A in the first 24 hours of enrollment. Vasoactive therapy initiation was earlier in group B as compared with group A (37 ± 10.14 vs. 47.33 ± 12.41 min) with lower fluid overload percentage (2.98% vs. 1.7%) in this group. However, there was no difference in time to shock resolution, 28-day ICU-free days, hospital-free days, and mortality.</p><p><strong>Conclusions: </strong>Advanced hemodynamic monitoring with electrocardiometry along with clinical assessment led to a restrictive fluid strategy in addition to minimizing the risk of fluid overload.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 4","pages":"e1242"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11960802/pdf/","citationCount":"0","resultStr":"{\"title\":\"Electrocardiometry for the Management of Pediatric Septic Shock: A Pilot Randomized Controlled Trial.\",\"authors\":\"Suman Sudha Moharana, Lalitha Av, Santu Ghosh\",\"doi\":\"10.1097/CCE.0000000000001242\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate the difference in the resuscitation fluid volume in the initial 6 hours in pediatric septic shock between those undergoing noninvasive continuous hemodynamic monitoring with electrocardiometry in addition to clinical monitoring vs. clinical monitoring alone.</p><p><strong>Design: </strong>Randomized control trial.</p><p><strong>Setting: </strong>PICU in a tertiary care hospital.</p><p><strong>Patients: </strong>Children from 2 months to 18 years with sepsis and unresolved shock after the initial fluid bolus (FB).</p><p><strong>Interventions: </strong>Children were randomized to one of the two groups, that is, electrocardiometry with clinical monitoring group (group B) and clinical monitoring alone group (group A). In group B, electrocardiometry variables (cardiac index and systemic vascular resistance index) along with clinical monitoring were used to guide FB, as well as selection and titration of vasoactive agents. Clinical parameters were used to initiate and titrate fluid resuscitation and vasoactive therapy in group A as per standard guidelines.</p><p><strong>Measurements and main results: </strong>One hundred nineteen children were enrolled in the study: 60 in group A and 59 in group B. There was a significantly higher requirement for resuscitation fluid volume (mean ± sd) within the initial 6 hours in the group A (30 ± 8.2 mL/kg) as compared with group B (22 ± 9.2 mL/kg). Similarly, maintenance along with resuscitation fluid volume (mean ± sd) administration (56 ±13 vs. 46 ±10.7, p < 0.001) was higher in group A in the first 24 hours of enrollment. Vasoactive therapy initiation was earlier in group B as compared with group A (37 ± 10.14 vs. 47.33 ± 12.41 min) with lower fluid overload percentage (2.98% vs. 1.7%) in this group. However, there was no difference in time to shock resolution, 28-day ICU-free days, hospital-free days, and mortality.</p><p><strong>Conclusions: </strong>Advanced hemodynamic monitoring with electrocardiometry along with clinical assessment led to a restrictive fluid strategy in addition to minimizing the risk of fluid overload.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 4\",\"pages\":\"e1242\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-03-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11960802/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001242\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001242","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Electrocardiometry for the Management of Pediatric Septic Shock: A Pilot Randomized Controlled Trial.
Objectives: To evaluate the difference in the resuscitation fluid volume in the initial 6 hours in pediatric septic shock between those undergoing noninvasive continuous hemodynamic monitoring with electrocardiometry in addition to clinical monitoring vs. clinical monitoring alone.
Design: Randomized control trial.
Setting: PICU in a tertiary care hospital.
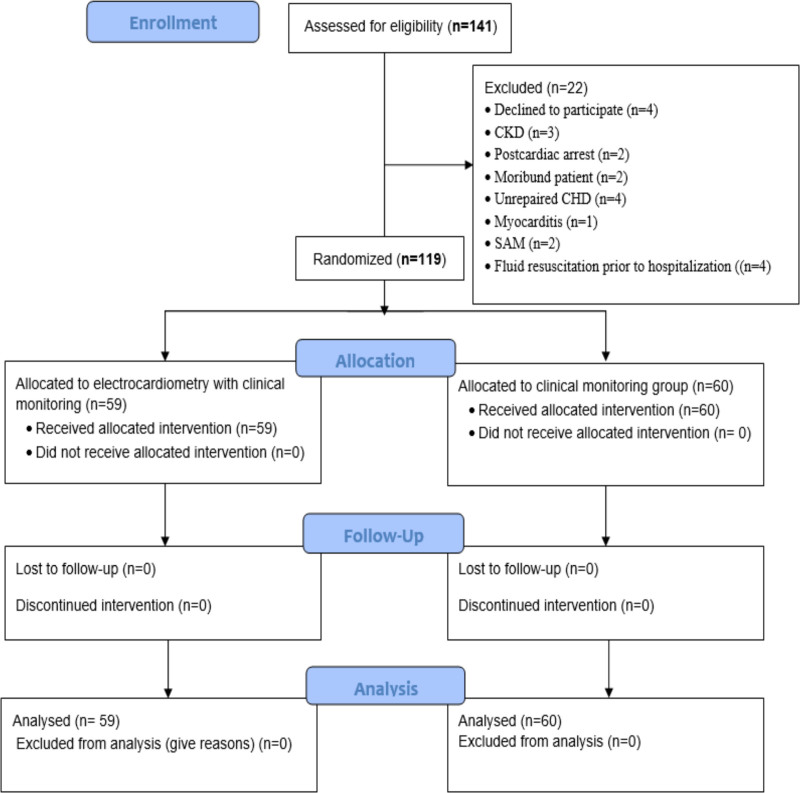
Patients: Children from 2 months to 18 years with sepsis and unresolved shock after the initial fluid bolus (FB).
Interventions: Children were randomized to one of the two groups, that is, electrocardiometry with clinical monitoring group (group B) and clinical monitoring alone group (group A). In group B, electrocardiometry variables (cardiac index and systemic vascular resistance index) along with clinical monitoring were used to guide FB, as well as selection and titration of vasoactive agents. Clinical parameters were used to initiate and titrate fluid resuscitation and vasoactive therapy in group A as per standard guidelines.
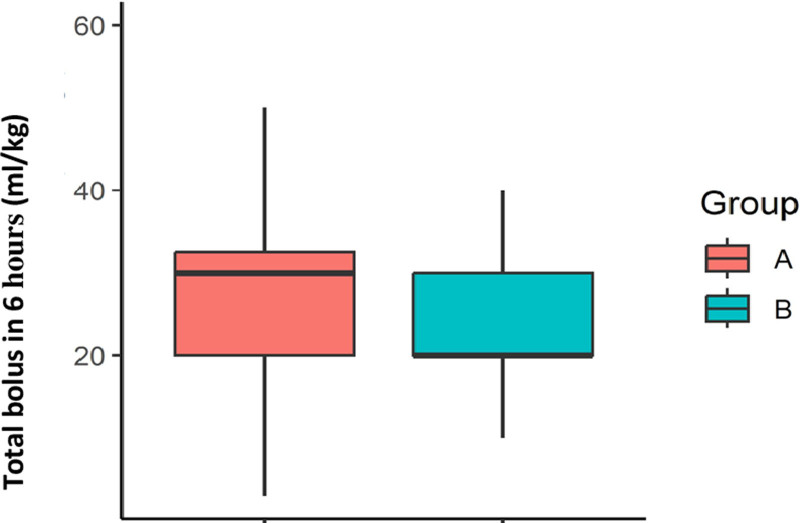
Measurements and main results: One hundred nineteen children were enrolled in the study: 60 in group A and 59 in group B. There was a significantly higher requirement for resuscitation fluid volume (mean ± sd) within the initial 6 hours in the group A (30 ± 8.2 mL/kg) as compared with group B (22 ± 9.2 mL/kg). Similarly, maintenance along with resuscitation fluid volume (mean ± sd) administration (56 ±13 vs. 46 ±10.7, p < 0.001) was higher in group A in the first 24 hours of enrollment. Vasoactive therapy initiation was earlier in group B as compared with group A (37 ± 10.14 vs. 47.33 ± 12.41 min) with lower fluid overload percentage (2.98% vs. 1.7%) in this group. However, there was no difference in time to shock resolution, 28-day ICU-free days, hospital-free days, and mortality.
Conclusions: Advanced hemodynamic monitoring with electrocardiometry along with clinical assessment led to a restrictive fluid strategy in addition to minimizing the risk of fluid overload.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


